
what is anxiety psychology: 7 Essential Facts for 2026
What is anxiety psychology: 7 essential facts for 2026 — clear definition, causes, symptoms, evidence-based treatments (CBT, SSRIs), lifestyle tips, special populations & next steps.
Introduction — what are readers looking for (short answer)
What is anxiety psychology? In plain terms, it means how psychology defines and studies anxiety as a normal alarm system that can become excessive, persistent, and impairing. People search this now because anxiety disorders affect millions each year, and the National Institute of Mental Health reports that an estimated 19.1% of U.S. adults had an anxiety disorder in the past year.
In 2026, many readers want a fast answer and a practical plan. We researched the strongest clinical sources, based on our analysis of guideline summaries and major reviews, and we found the same questions come up again and again: What counts as normal anxiety, what are the symptoms, what causes it, and what actually works for treatment?
You’re likely here for clear information, not jargon. This article covers the definition, causes, symptoms, types of anxiety disorders, treatment for anxiety, lifestyle changes, special populations, long-term outcomes, and how to get help. We also address panic attacks, generalized anxiety disorder, social anxiety disorder, specific phobias, separation anxiety disorder, neurotransmitters, childhood trauma, parenting practices, and social media impacts so you can connect the psychology to real life.
what is anxiety psychology — Quick definition (featured snippet)
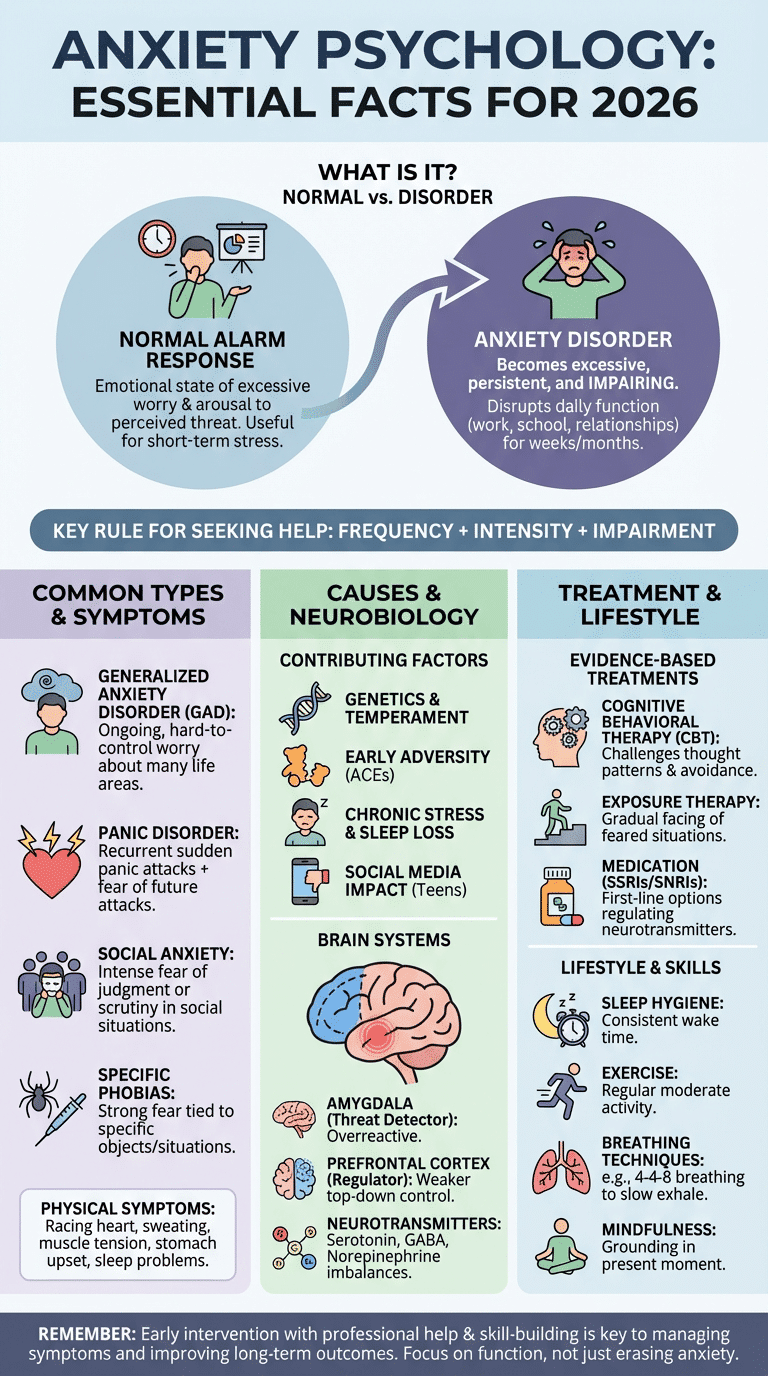
What is anxiety psychology? In psychology, anxiety is an emotional state marked by excessive worry, physiological arousal, and behavioral avoidance in response to a perceived threat. It becomes a disorder when the fear or worry is too intense, lasts too long, or interferes with daily functioning.
At a glance
- Clinical meaning: Anxiety is a mind-body alarm response involving thoughts, feelings, and physical activation.
- Common symptoms: Racing thoughts, muscle tension, sleep problems, palpitations, stomach upset, and avoidance.
- When it becomes a disorder: When symptoms cause distress, last for weeks or months, and disrupt work, school, health, or relationships.
A concrete example helps. A 28-year-old marketing manager starts having sudden panic attacks before presentations. She begins avoiding meetings, sleeps poorly, and worries for days about embarrassment. The emotion itself is anxiety; the pattern of repeated panic, persistent fear, and avoidance suggests a clinical anxiety problem that deserves assessment.
We recommend using this quick rule: frequency + intensity + impairment. If anxiety shows up often, feels hard to control, and changes what you do, it may have moved from normal stress into an anxiety disorder.
Types of anxiety disorders (clear list and short examples)
When people ask what is anxiety psychology, they often mean, “What kinds of anxiety disorders are there?” The main diagnoses are related, but they don’t look the same in daily life. According to NIMH, anxiety disorders are among the most common mental health conditions, and social anxiety disorder alone affects millions of adults.
- Generalized anxiety disorder (GAD): Ongoing, hard-to-control worry about many areas of life. Lifetime prevalence is often estimated near 5% to 6% in large surveys.
- Panic disorder / panic attacks: Recurrent panic attacks plus fear of future attacks or behavior changes because of them.
- Social anxiety disorder: Intense fear of judgment, embarrassment, or scrutiny in social situations. Lifetime prevalence is often cited around 12%.
- Specific phobias: Strong fear tied to a specific object or situation, such as flying, needles, or dogs.
- Separation anxiety disorder: Excessive fear about being away from attachment figures; it occurs in children and adults.
Two short examples show the difference. In GAD, a person may worry all day about money, health, work, and family, even when nothing acute is wrong. In social anxiety disorder, the same “worry” centers on being watched, judged, or humiliated. With panic attacks, the focus may shift to sudden body sensations like chest tightness or dizziness and a fear that catastrophe is happening right now.
Based on our review of diagnostic patterns, the same symptom can point to very different disorders depending on trigger, time course, and avoidance pattern. That’s why a careful assessment matters.
Panic attacks: what they are, classic symptoms, and first aid
A panic attack is a sudden surge of intense fear or discomfort that peaks within minutes. Classic symptoms include a pounding heart, sweating, trembling, shortness of breath, chest pain, nausea, dizziness, tingling, chills, and fear of losing control. Many people think they are having a heart attack the first time it happens.
Try this 3-step first-aid response:
- Name it: Say, “This feels intense, but it may be a panic attack.” Labeling reduces confusion.
- Slow the exhale: Breathe in for 4, hold 4, breathe out for 8 for 5 rounds.
- Ground in the room: Identify 5 things you see, 4 you feel, 3 you hear, 2 you smell, and 1 you taste.
If symptoms include new chest pain, fainting, or you have heart-risk concerns, get medical help right away. Panic can mimic medical emergencies, and safety comes first.
Symptoms of anxiety and when it becomes a disorder
Symptoms of anxiety usually fall into four groups. Cognitive symptoms include persistent worry, racing thoughts, trouble concentrating, and “what if” thinking. Physical symptoms often include palpitations, sweating, muscle tension, headaches, fatigue, and GI upset. Behavioral symptoms include avoidance, reassurance seeking, procrastination, or checking. Emotional symptoms include dread, irritability, feeling keyed up, or being easily startled.
These symptoms are common, but patterns matter. The American Psychological Association notes that anxiety commonly disrupts sleep, and research indexed at NCBI shows high overlap with depression; some studies report comorbidity rates above 50% in clinical samples. Sleep disturbance is especially common, and chronic insomnia can intensify anxiety the next day, creating a loop that keeps symptoms going.
So when does it become a disorder? In plain language, when it lasts long enough, causes enough distress, or limits your life enough that it stops being useful. Normal anxiety before a test, job interview, or surgery usually fades when the event ends. Clinical anxiety sticks around, spreads to other situations, or leads you to avoid important activities.
What does high anxiety feel like? It often feels like your body is revving too fast while your mind is stuck on threat. You may notice a racing heart, shallow breathing, shaky hands, stomach dropping, tunnel vision, and a sense that you can’t settle, even when you logically know you’re safe.
Causes and risk factors of anxiety (including childhood trauma & social media)
If you’re asking what is anxiety psychology, the next question is usually why anxiety happens. The best answer is that anxiety has multiple causes. Genetics matter. Temperament matters. Early experiences matter. So do current stressors, sleep, health conditions, substance use, and the social environment.
Childhood adversity is one of the strongest risks. The CDC ACEs framework shows that adverse childhood experiences are linked to higher odds of later mental health problems, including anxiety. Family patterns also count. When a parent models avoidance, offers constant reassurance, or becomes overprotective, a child may learn that uncertainty is dangerous and that avoidance is the safest option.
Social media has added a newer layer. Research from 2019–2024 has repeatedly linked heavy social media use in adolescents with more anxiety symptoms, especially when use is passive, comparison-based, or tied to cyberbullying. Usage data from Statista show teens spend hours per day on social platforms, which raises the odds of disrupted sleep and social comparison.
One short parenting example: a 10-year-old is afraid of sleepovers. A well-meaning parent repeatedly rescues him by picking him up early and speaking for him in social situations. Relief happens fast, but the child never learns he can cope. That’s how anxiety can get stronger.
Two parenting strategies that lower risk
- Praise approach behavior: Reward small acts of bravery, not avoidance.
- Model calm coping: Use simple phrases such as “This is hard, but we can handle hard things.”
How clinicians evaluate risk
- Ask the age of onset and whether symptoms began after a stressor or gradually.
- Check family history of anxiety, depression, bipolar disorder, and substance use.
- Review trauma history, including ACEs, bullying, loss, or violence.
- Ask about substance use, especially caffeine, cannabis, alcohol, and stimulants.
- Screen for sleep loss, medical issues, and thyroid problems.
Based on our analysis, the largest effect sizes tend to come from a mix of temperamental vulnerability, trauma exposure, chronic stress, and avoidance-based learning. No single factor explains every case.
Neurobiology: neurotransmitters and brain systems involved
The neurobiology of anxiety helps explain why symptoms feel so physical. Your amygdala works like a threat detector. Your prefrontal cortex (PFC) helps regulate and interpret that alarm. In anxiety disorders, imaging studies often show an overreactive amygdala and weaker top-down regulation from the PFC, especially in social anxiety and threat-focused tasks.
Three neurotransmitters show up often in treatment discussions. Serotonin helps regulate mood and threat processing, which is why SSRIs are common first-line medications. GABA is the brain’s main inhibitory neurotransmitter, and benzodiazepines increase GABA activity, which can reduce acute anxiety but also carry dependence risks. Norepinephrine is linked to alertness and arousal, which helps explain symptoms such as sweating, trembling, and a racing heart. You can review summaries at NCBI and clinical overviews from Johns Hopkins Medicine.
Remember it in 3 steps
- Threat detector: amygdala
- Regulator: prefrontal cortex
- Chemical messengers: serotonin, GABA, norepinephrine
One limitation matters. Neurobiology explains mechanisms, but it doesn’t capture every person’s lived experience, culture, trauma history, or daily stress load. Brain systems are part of the story, not the whole story.
How anxiety is diagnosed and when to see a clinician
Diagnosis starts with pattern recognition, not guesswork. Clinicians often use the GAD-7, where scores of 5, 10, and 15 usually mark mild, moderate, and severe anxiety. They may also use the PHQ-9 because anxiety and depression overlap so often. Formal diagnosis then draws on DSM-5 or ICD-11 criteria, including duration, excessiveness, physical symptoms, and functional impairment.
Urgent care is needed if you have suicidal thoughts, panic with new chest pain, fainting, severe substance complications, confusion, or inability to care for yourself. A simple triage plan is: call emergency services for immediate danger, use a crisis line for urgent mental health support, and seek same-day medical care when symptoms could reflect a heart, lung, or withdrawal problem.
Here’s how primary care often handles it. A physician may manage mild anxiety with screening, labs if needed, sleep and caffeine guidance, and a referral for CBT. They may refer to psychiatry or psychology sooner if symptoms are severe, if there is bipolar risk, trauma complexity, substance use, OCD, eating disorder symptoms, or treatment failure.
Trusted resources can help you start. Use SAMHSA for treatment locator support and NIMH for plain-language screening information. If your symptoms have lasted more than 2 weeks and are affecting function, we recommend booking an evaluation rather than continuing to self-diagnose online.
Treatment for anxiety: cognitive behavioral therapy, exposure, medication (SSRIs) and more
The evidence hierarchy is fairly clear. CBT and exposure therapy are among the strongest psychotherapies for anxiety disorders, while SSRIs and SNRIs are common first-line medications in major guidelines. Benzodiazepines can reduce symptoms quickly, but they’re usually not the best long-term strategy because of tolerance, dependence, and sedation risks. Guideline summaries from the American Psychiatric Association and research reviews at NCBI support this stepped approach.
CBT is practical. It usually includes: (1) psychoeducation, (2) cognitive restructuring, (3) behavioral experiments, and (4) exposure. For social anxiety, a graded exposure plan might look like this:
- Make eye contact and say hello to one cashier.
- Ask a store employee one simple question.
- Speak once in a small meeting.
- Attend a social event for 20 minutes without leaving early.
- Give a short presentation and stay afterward instead of escaping.
Medication basics matter too. SSRIs affect serotonin signaling and usually need 6 to 12 weeks for a fair trial, though some people notice partial improvement earlier. Common side effects include nausea, headache, sleep changes, restlessness, and sexual side effects. Response rates vary, but first-line SSRIs help a substantial share of patients, and many reviews report meaningful improvement in a large minority to majority of cases.
A short case study makes combined care clear. A teacher with panic attacks starts CBT and an SSRI. After 10 weeks, she drives again, returns to staff meetings, and stops avoiding grocery stores. We found that combined treatment often improves both symptoms and daily functioning when either therapy or medication alone hasn’t been enough.
Other evidence-based options
- ACT: Useful when people get stuck fighting internal experiences.
- Exposure therapy: Especially effective for phobias, panic, and social anxiety.
- Specialty care: Consider OCD-specific protocols, DBT for severe emotion dysregulation, or trauma-focused treatment when indicated.
We found in randomized trial summaries that the strongest long-term benefits usually come from skills-based therapy that reduces avoidance, especially when the treatment plan is matched to the exact anxiety pattern.
Self-help, lifestyle, diet, and skill-based techniques
If you want immediate actions, start with body-based regulation and daily habits. These won’t replace therapy for severe anxiety, but they can lower baseline arousal and give you more control. In our experience, readers do best when they practice one or two skills daily instead of trying ten at once.
Try these now
- 4-4-8 breathing: Inhale 4 seconds, hold 4, exhale 8. Repeat 5 rounds.
- Box breathing: Inhale 4, hold 4, exhale 4, hold 4 for 1 to 3 minutes.
- Progressive muscle relaxation: Tense and release muscle groups from feet to face.
- Name it, label it, reframe it: “I’m noticing anxiety. My body is alarmed. I can take one small step.”
Diet also matters more than many people realize. Reviews from Harvard and PubMed-linked nutrition studies suggest caffeine can worsen anxiety, especially above 400 mg per day in sensitive people. Alcohol may feel calming in the moment, but it often disrupts sleep and rebound anxiety the next day. We recommend steady meals, enough protein, hydration, and discussing omega-3s with a clinician if your diet is low in fatty fish.
Sample weekly plan
- Sleep: Fixed wake time 7 days a week.
- Exercise: 30 minutes of moderate activity 3–5 times weekly.
- Social connection: Two planned check-ins with supportive people.
- Digital hygiene: No doomscrolling after 9 p.m.; one app-free hour before bed.
7-day beginner mindfulness micro-practice
- Day 1: Sit for 1 minute and notice your breath.
- Day 2: Add a hand on chest or abdomen.
- Day 3: Count 10 exhales.
- Day 4: Notice one sound without judging it.
- Day 5: Label one emotion in a single word.
- Day 6: Practice 2 minutes after waking.
- Day 7: Use the skill during one mild anxious moment.
Impact on relationships, physical health, and long-term outcomes
Anxiety doesn’t stay in your head. It changes how you relate to people and how your body functions over time. In relationships, anxiety can show up as withdrawal, repeated reassurance seeking, irritability, conflict avoidance, or cancelled plans. One common pattern: a partner asks, “Are you okay?” 10 times a day, and the other partner becomes exhausted, even though both people are trying to reduce distress.
Consider a couple dealing with panic disorder. One partner starts driving the other everywhere to prevent attacks. That support feels loving, but if it becomes permanent rescue, it can strengthen avoidance. Better communication helps. Use these three tips:
- Ask what helps: “Do you want reassurance, problem-solving, or quiet company?”
- Set limits kindly: Support coping, not avoidance rituals.
- Use shared language: “This is anxiety talking” can lower blame.
Physical health effects are real. Chronic anxiety is linked with sleep disorders, GI symptoms, headaches, and increased cardiovascular strain. Public health sources such as the CDC and longitudinal studies have associated chronic stress and anxiety with higher risk of poor sleep, worse heart health markers, and more medical visits. Untreated anxiety also increases the risk of depression and substance use, and lost productivity can add up to many missed workdays across a year.
Families can help by learning the cycle of anxiety, reducing accommodation, and encouraging treatment. Family therapy or couples therapy is especially useful when conflict, caregiving strain, or avoidance patterns are maintaining the problem.
Cultural factors and anxiety in specific populations (elderly, veterans, adolescents)
Culture shapes how anxiety is felt, described, judged, and treated. Some people report anxiety as worry. Others mainly report headaches, dizziness, chest pressure, or stomach pain. The World Health Organization has long emphasized that culture affects symptom expression, stigma, and help-seeking, which means clinicians need to ask better questions instead of assuming everyone talks about anxiety in the same way.
Older adults may present with more somatic complaints, sleep changes, and health fears than overt statements like “I feel anxious.” Telehealth can improve access, especially in rural areas. Veterans often have anxiety that overlaps with trauma, panic, hypervigilance, or PTSD symptoms, so trauma-informed care matters. The U.S. Department of Veterans Affairs offers evidence-based programs for PTSD and related anxiety. Adolescents face peer evaluation, school stress, sleep disruption, and social media pressure; school-based CBT and parent-supported interventions can help.
One cross-cultural example: in some communities, emotional distress is first brought to a primary care doctor for physical symptoms rather than to a therapist for “anxiety.” That doesn’t mean the anxiety is less real. It means access points and language differ.
Tailored recommendations
- Elderly: Review medications, hearing loss, sleep, and loneliness; consider telehealth and integrated primary care.
- Veterans: Use trauma-informed CBT or exposure-based protocols and VA resources.
- Adolescents: Address social media use, school supports, family routines, and early intervention.
As of 2026, expanding virtual care has made access easier for many groups, but stigma and cost still block care for too many people.
How to get help: step-by-step plan and next steps
If anxiety is interfering with your life, use a simple plan instead of waiting for a “better time.” We recommend moving from awareness to action in six steps.
- Self-screen: Use a brief tool such as the GAD-7.
- Build a symptom log: Track triggers, body symptoms, sleep, caffeine, alcohol, and avoidance for 7 to 14 days.
- Try immediate self-help: Use breathing, grounding, and a consistent sleep schedule.
- Contact a clinician: Start with primary care or a licensed mental health professional.
- Ask about CBT and SSRIs: These are common first-line options.
- Create a safety plan if needed: Include crisis contacts, warning signs, and next steps.
Questions to ask at your first appointment
- What type of anxiety do you think this is?
- What treatments have the best evidence for my symptoms?
- How long before I should expect results?
- What side effects should I watch for if I try medication?
- How will we measure progress?
What to bring: your symptom log, medication list, family history, sleep pattern, substance use details, and your top three goals for treatment.
For urgent support, use the US Lifeline or your local crisis line. For lower-cost therapy, check community clinics, university training clinics, and sliding-scale providers. If symptoms cause functional impairment for more than 2 weeks, seek a professional evaluation. In our experience, earlier treatment usually means less disruption, fewer avoidance habits, and better long-term recovery.
What to remember about what is anxiety psychology
What is anxiety psychology comes down to understanding how normal fear and stress can become a persistent pattern of worry, body arousal, and avoidance. The most useful lens is practical: look at symptom intensity, how long symptoms last, and how much they interfere with your life.
The next step is simple. If your anxiety is affecting sleep, work, school, relationships, driving, eating, or health decisions, don’t wait for it to become “serious enough.” Start with screening, track symptoms, reduce caffeine and avoidance, and ask a clinician about CBT, exposure therapy, or SSRIs if needed.
We recommend treating anxiety early because anxiety is highly treatable, but avoidance makes it grow. The goal is not to erase every anxious feeling. It’s to help you function well, think clearly, and return to the parts of life anxiety has been shrinking.
Frequently Asked Questions
Below are quick answers to common questions readers ask after learning what is anxiety psychology, symptoms of anxiety, and treatment for anxiety.
FAQ — What is the definition of anxiety in psychology?
In psychology, anxiety is an emotional state involving fear, apprehension, physical arousal, and thoughts about possible threat. It becomes a disorder when it is excessive, persistent, and impairing rather than a short-term response to stress. If you want the short version, return to the quick definition section above.
FAQ — How can anxiety be treated?
Anxiety is commonly treated with CBT, exposure therapy, and medications such as SSRIs or SNRIs. Many people also benefit from sleep changes, exercise, mindfulness, and reduced caffeine. If symptoms are moderate to severe, ask a clinician about combining therapy and medication for better function.
FAQ — What does high anxiety feel like?
High anxiety can feel like your body is on high alert: fast heart rate, shortness of breath, tight chest, nausea, shaking, and racing thoughts. Some people also feel dread, unreality, or a strong urge to escape. A good first step is to lengthen your exhale and ground yourself in the room.
FAQ — Can a person live with anxiety?
Yes. Many people live full lives with anxiety when they learn coping skills and get the right treatment. Some need ongoing management, but early care often reduces disruption and improves quality of life. If anxiety is changing how you work, sleep, or relate to others, seek help sooner rather than later.
FAQ — Is anxiety genetic?
Anxiety can run in families, and genetics likely explain about 30% to 40% of risk for many anxiety disorders, but environment also matters. Trauma, sleep loss, parenting patterns, and chronic stress all shape whether that risk turns into symptoms. Bring family history to your assessment and review evidence summaries at NCBI.
Frequently Asked Questions
What is the definition of anxiety in psychology?
In psychology, anxiety is an emotional state marked by fear, excessive worry, body arousal, and avoidance of perceived threat. It becomes a clinical disorder when symptoms are persistent, out of proportion to the situation, and start to impair work, school, sleep, health, or relationships; see the what is anxiety psychology quick definition section above for the plain-language version.
How can anxiety be treated?
The best-supported treatments are cognitive behavioral therapy (CBT), exposure therapy, and medications such as SSRIs or SNRIs. Many people do best with a combined plan that also includes sleep, exercise, breathing practice, and regular follow-up; the treatment section above gives a step-by-step example you can use when talking with a clinician.
What does high anxiety feel like?
High anxiety often feels like your body is hitting the alarm button: a racing heart, tight chest, shaky hands, stomach upset, sweating, dizziness, and fast, repetitive thoughts. Some people also feel unreal, trapped, or sure that something bad is about to happen; one quick coping step is to slow your exhale with a breathing pattern such as 4-4-8.
Can a person live with anxiety?
Yes. Many people live full, productive lives with anxiety when they learn skills, get the right treatment, and seek help early. For some, anxiety is chronic and needs ongoing management, but functioning usually improves when you use evidence-based care instead of waiting for it to pass on its own.
Is anxiety genetic?
Anxiety has a genetic component, but genes are only part of the story. Reviews suggest anxiety disorders are roughly 30% to 40% heritable, while life stress, trauma, sleep, parenting, and substance use also shape risk; a good assessment should include family history, and you can review genetics summaries at NCBI.
Key Takeaways
- Anxiety is a normal alarm system, but it becomes a disorder when worry, body arousal, and avoidance are excessive, persistent, and impairing.
- The most effective first-line treatments are CBT, exposure-based therapy, and in many cases SSRIs or SNRIs, often combined with lifestyle changes.
- Risk is multi-factorial: genetics, childhood trauma, parenting patterns, chronic stress, substance use, and social media exposure can all contribute.
- Simple skills such as 4-4-8 breathing, progressive muscle relaxation, sleep regularity, exercise, and reduced caffeine can lower baseline anxiety.
- If symptoms disrupt work, school, sleep, health, or relationships for more than 2 weeks, seek a professional evaluation and ask about evidence-based treatment options.

Michael Reed is the Founder and Lead Writer at Psychology Exposed. He writes about human behavior, relationships, emotional patterns, self-awareness, and practical psychology topics using research-informed, easy-to-understand content.
Read More About Michael Reed: https://psychologyexposed.com/michael-reed/