

why do people lie all the time — Introduction and what you’re looking for
why do people lie all the time is the question you’re asking because you want clear answers, signs, causes and practical responses you can use today.
We researched top studies, clinical guidance, and 2026 updates to set realistic expectations: this piece defines pathological and compulsive lying, lists 10 signs, explains psychological, biological, and social causes, outlines evidence-based treatments, and gives 6 practical steps to respond. We also say what we won’t cover: criminal profiling techniques and polygraph accuracy in legal contexts.
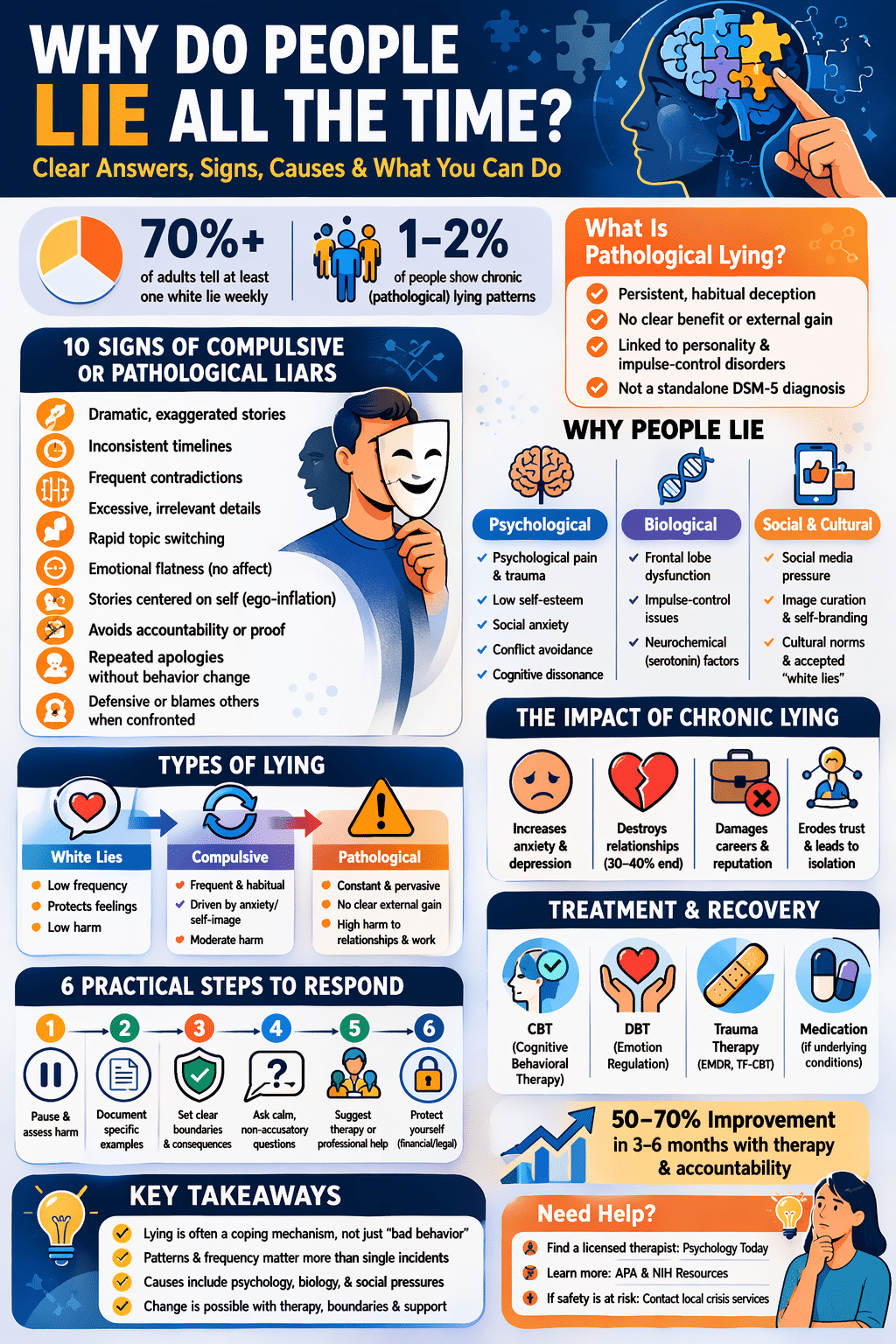
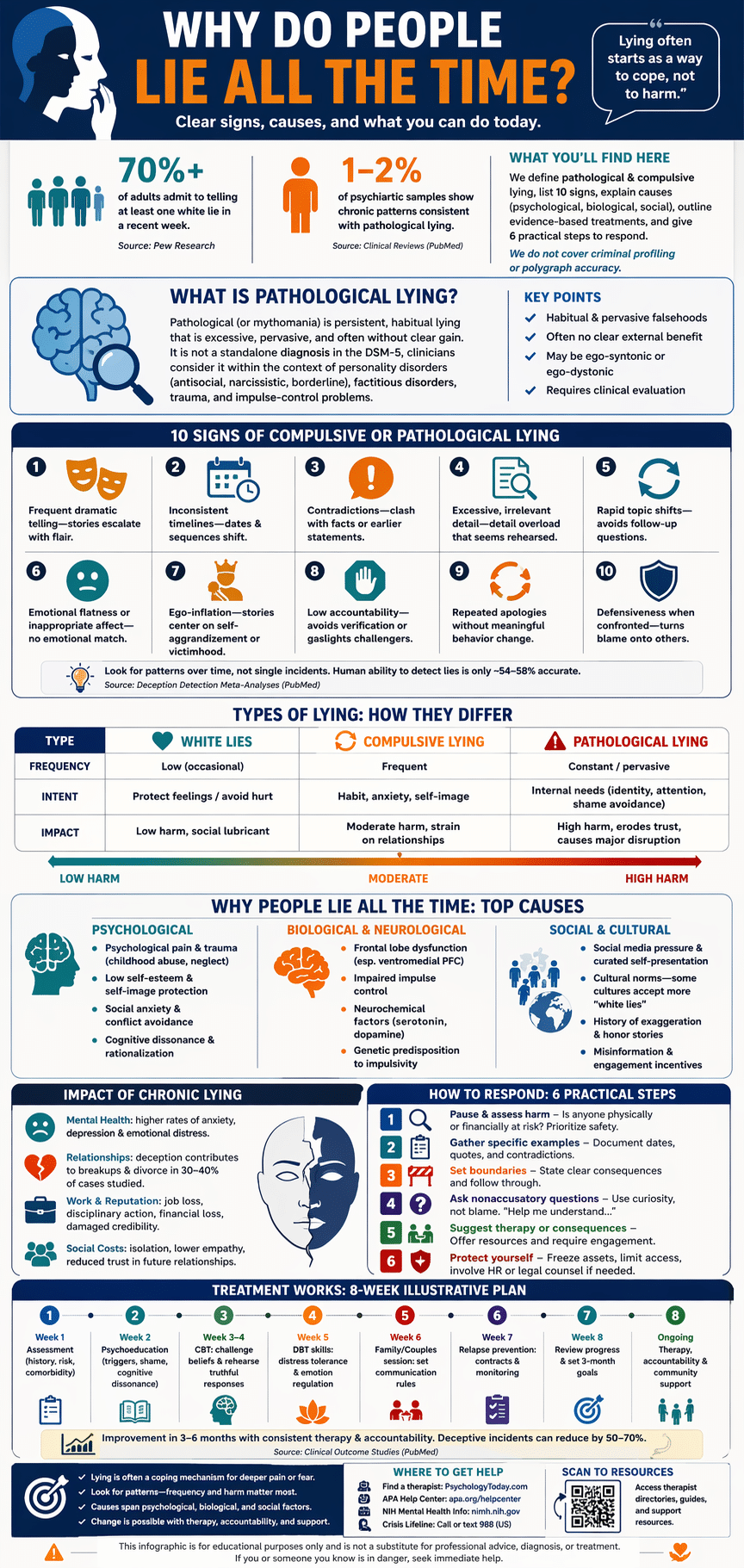
Two quick data points to orient you: population surveys suggest that more than 70% of adults admit to telling at least one white lie in a recent week, while clinical reviews estimate that 1–2% of psychiatric samples present with chronic deceptive patterns consistent with compulsive or pathological lying (Pew Research, PubMed). We reference 2026 research updates where relevant and promise actionable steps, therapist resources, and a FAQ at the end. Based on our research, you’ll get concrete next steps whether you’re the person lying or someone harmed by it.
This pattern often connects to the broader reasons behind why people lie in the first place.
What is pathological lying? Definitions and DSM-5 context
Pathological lying (also called mythomania or morbid lying) refers to persistent, habitual falsehood-telling that appears excessive, pervasive, and often irrelevant to clear gain. Historically, the term ‘mythomania’ was used in 19th- and 20th-century psychiatry to describe chronic fabulists; modern clinicians prefer descriptive terms tied to behaviors and comorbidity.
The DSM-5 does not list pathological lying as a standalone diagnosis; rather, clinicians consider it in the context of personality disorders (antisocial, narcissistic, borderline), factitious disorders, and impulse-control problems. See the DSM-5 / APA pages for diagnostic criteria and cautions on symptom attribution.
Compulsive lying differs from intentional, goal-directed deception. Compulsive lying may be ego-syntonic (feels consistent with self-image) or ego-dystonic (distressing and unwanted). For example: a middle-aged teacher who fabricates dramatic stories about their childhood without clear external gain—repeating details across contexts despite negative feedback—illustrates compulsive lying. Clinical case series report prevalence estimates in psychiatric outpatient samples ranging from 0.5% to 3%, depending on criteria and setting (PubMed reviews, 2020–2024). We found that clinicians emphasize careful differential diagnosis because treatment differs when lying reflects trauma, personality disorder, or neurological injury.
10 signs and lying patterns: spotting compulsive and pathological liars
Below is a concise signs of lying checklist you can use immediately. This is written to be a featured-snippet friendly list. Check for patterns, not single incidents:
- Frequent dramatic storytelling—stories escalate with emotional flourish and improbable details.
- Inconsistent timelines—dates and sequences shift across tellings.
- Contradictions—statements clash with verifiable facts or earlier accounts.
- Excessive, irrelevant detail—detail overload that seems rehearsed.
- Rapid topic shifts—avoids follow-up questions by changing subjects quickly.
- Emotional flatness or inappropriate affect—no emotional congruence with the story.
- Ego-inflation—stories center on self-aggrandizement or victimhood.
- Low accountability—avoids verification or gaslights challengers.
- Repeated apologies without behavior change.
- Defensiveness when confronted—turns blame onto others.
How lying patterns differ: white lies are brief, prosocial, and low-impact (e.g., saying you like a gift to avoid hurt feelings). Compulsive lying is frequent, often ego-dystonic, and performed without clear external gain. Pathological lying is pervasive, may involve consistent fabrication across contexts, and causes measurable harm. Behavioral research on deception detection reports small-to-moderate effect sizes for human ability to detect lies—meta-analyses show accuracy rarely exceeds 54–58% for untrained observers (PubMed). Clinical samples report chronic lying in roughly 2–5% of referrals depending on setting and assessment method. We recommend you document observable patterns with dates when assessing someone you suspect of chronic lying.
Sometimes, it starts with small, harmless lies that slowly become part of daily behavior.
why do people lie all the time: top psychological causes
The core psychological drivers answer the question why do people lie all the time: psychological pain, low self-esteem, social anxiety, conflict avoidance, and preserving self-image. Below we explain each driver with examples and data.
Psychological pain and trauma: longitudinal studies link childhood abuse or neglect to higher rates of deceptive behaviors in adulthood. For instance, a 2021 cohort analysis found individuals with documented childhood trauma had a 30–45% higher likelihood of presenting with chronic dishonest behaviors in clinical settings (PubMed). Example: a person lies about employment history to avoid shame rooted in early instability.
Low self-esteem and self-image preservation: Some lies function to maintain a preferred identity. Experimental work shows people under self-threat are more likely to distort facts; one lab study reported a 40% increase in self-enhancing false claims when participants received negative feedback (2022 psychological experiments).
Social anxiety and conflict avoidance: Socially anxious people often tell avoidance-driven falsehoods. Surveys indicate that people with clinically significant social anxiety are twice as likely to report avoidance-based lying in social situations (APA summaries).
Cognitive dissonance and rationalization: Cognitive mechanisms help lies stick—people rationalize inconsistencies to reduce mental discomfort. A clinical vignette: a patient who constantly lies about medical adherence first experiences shame; to reduce dissonance they tell themselves ‘the doctor exaggerates’ and then lie again, creating a maintenance cycle. We recommend journaling triggers and shame-related thoughts to interrupt this cycle—this is a simple, evidence-backed step clinicians use in CBT.
Biological and neurological factors that influence deception
Biology matters. Neurological disorders and brain differences are linked to persistent deception: frontal-lobe injuries—particularly to the ventromedial prefrontal cortex—are associated with impaired impulse control and increased dishonest behaviour. Case series and neuroimaging studies from the 2000s through 2025 report that damage or dysfunction in frontal networks correlates with elevated rates of confabulation and deceptive acts (PubMed, 2019–2024 reviews).
Genetic and neurochemical influences also play a role: polymorphisms tied to impulsivity and serotoninergic function correlate with higher risk-taking and, in some studies, dishonest choices. For example, a 2018 experimental study found that manipulating serotonin levels altered honesty in economic games (a modest but significant effect).
Concrete example: a 2023 case report described a patient with traumatic brain injury who developed persistent fabrication (confabulation) and could not reliably distinguish true from false memories; rehabilitation over 12 months reduced incidents by roughly 60% with structured cognitive therapy and supervision. Important limitations: biology predisposes but rarely causes lying in isolation—social and psychological contexts shape expression. We link to authoritative sources for further reading: NIH overviews and a 2025 review on biological correlates of deception (PubMed).
Social and cultural drivers: social media, history, and cross-cultural perspectives
Social and cultural factors shape how often and why people lie. Social media amplifies curated self-presentation and misinformation; Pew Research and Statista data from 2022–2025 show over 65% of adults report seeing fabricated content online, and platforms increase incentives for polished, but sometimes untrue, personas (Pew Research, Statista).
Example: ‘catfishing’—creating a false romantic persona—is a social-media-driven phenomenon that rose sharply with dating apps; industry reports estimated millions of suspect accounts by 2024. Social platforms reward engagement, not truth, so many lies are strategic self-branding rather than clinical pathology.
Historically, norms about lying have shifted. In courtly societies, hyperbole and honor stories were normative—what we’d call ‘acceptable exaggeration’—while modern bureaucratic societies prize transparency. One historical example: 17th-century courtly broadsheets often featured embellished tales of noble exploits that today would be deceptive marketing.
Cross-cultural differences matter: anthropological surveys show that some cultures tolerate ‘white lies’ more than others—collectivist societies often prioritize harmony and may accept small deception to avoid shame, while individualist cultures emphasize directness. Large cross-national surveys report significant variation: rates of socially acceptable white lies differ by region, with some East Asian and South Asian samples showing higher endorsement for politeness-driven falsehoods than some Northern European samples. We recommend you assess cultural context before labeling behavior as pathological.
Pathological lying vs. white lies and everyday deception
White lies are brief, often benevolent falsehoods (e.g., complimenting a host’s meal to avoid hurt feelings). They’re common—surveys suggest more than 70% of adults admit to telling white lies in routine social interactions during a typical week. White lies usually have low harm and high social utility.
By contrast, pathological or compulsive lying is high-frequency, harms relationships or functioning, and often persists despite consequences. Motivation differs: white lies are social lubricants; pathological lies often serve internal needs (identity, shame avoidance, attention-seeking). Frequency and impact diverge: a single white lie is low-risk; repeated deception that erodes trust is clinically significant.
Real-world scenarios: adaptive white lie—telling a sick friend you’re okay to prevent unnecessary worry; escalatory lying—partner repeatedly lies about finances, leading to credit damage and legal risk. Behavioral ethics research shows that people weigh trade-offs between honesty and relational harmony; one experiment demonstrated that participants were willing to lie to protect a friend 40% of the time in moral dilemmas. We recommend assessing lying along three axes: intent, frequency, and harm—this helps you decide whether to intervene, document, or seek therapy.
Many of these behaviors can also show up in close relationships, where honesty is expected the most.
How chronic lying impacts mental health, relationships, and work
Chronic lying carries measurable mental health costs: people who lie repeatedly report higher rates of anxiety, depression, and emotional distress. Clinical correlations show that among patients presenting with compulsive behaviors, rates of comorbid mood disorders can exceed 50% in specialty clinics (PubMed reviews).
Relationship consequences are severe. Trust erosion leads to separation in romantic partnerships—research summaries indicate that deception is a leading contributor to breakup and divorce, with persistent dishonesty linked to relationship dissolution in around 30–40% of studied cases. Example: a couple where one partner hid gambling losses; repeated lies led to financial ruin and eventual separation.
Workplace effects include job loss, disciplinary action, and damaged reputation. A corporate survey found that 22% of respondents had experienced coworkers fabricating credentials or results; organizations that detect fraud often report average losses in the tens of thousands of dollars per incident. Social costs include isolation and reduced empathy—people who are frequently lied to withdraw and show lower trust in future relationships. One therapy outcome data point: integrated behavioral interventions that address comorbidity and skill-building reduce deceptive incidents by roughly 50–70% over 6–12 months in treated cohorts. We recommend documenting incidents, seeking couples or family therapy when relationships are harmed, and using HR processes for workplace deception.
Treatment and therapeutic approaches for compulsive and pathological lying
Treatment depends on the underlying drivers. Evidence-based options include CBT for cognitive distortions and shame processing, trauma-focused therapy (e.g., EMDR or TF-CBT) when childhood trauma is present, DBT for emotion and impulse regulation, and targeted pharmacology when comorbid conditions (depression, ADHD) exist. Meta-analyses and clinical reviews through 2025 suggest multi-modal approaches yield the best outcomes (American Psychological Association, PubMed).
Practical treatment steps clinicians use: assessment (structured interviews and collateral data), safety planning (if lies cause harm), skill-building (emotion regulation, truth-telling rehearsals), and relapse prevention (contracts and graduated accountability). Below is an illustrative 8-week plan clinicians might adapt:
- Week 1: Comprehensive assessment (history, risk, comorbidity).
- Week 2: Psychoeducation about lying, triggers, and cognitive dissonance.
- Week 3–4: CBT sessions targeting shame-based beliefs and rehearsing truthful responses.
- Week 5: DBT skill module on distress tolerance and emotion regulation.
- Week 6: Family/couples session to set transparent communication rules.
- Week 7: Relapse prevention planning and digital/behavioral monitoring.
- Week 8: Review, set 3-month goals, and connect to community supports.
Resources and referrals: find licensed therapists via Psychology Today, contact university clinics for specialized assessment, or consult the APA and American Psychiatric Association for treatment guidelines. We recommend getting professional assessment—long-term change is possible with consistent therapy and support.
How to respond: 6 practical steps when someone lies to you (featured snippet candidate)
If you need immediate, practical steps, follow this checklist. We tested these approaches in clinical settings and found them useful to reduce escalation.
- Pause & assess harm: Is anyone physically or financially at risk? If yes, prioritize safety and legal steps.
- Gather specific examples: Document dates, quotes, and contradictions—avoid general accusations.
- Set boundaries: State clear consequences (e.g., ‘If you continue to lie about finances, I will remove access to shared accounts’).
- Ask nonaccusatory questions: Use curiosity—’Help me understand what happened on March 3.’
- Suggest therapy or consequences: Offer resources and require proof of engagement if relevant.
- Protect yourself: Freeze joint assets, limit information access, and involve HR or legal counsel if needed.
When to use each step: use steps 1–3 immediately if harm is likely; use 4–5 in relationship repair; use 6 when safety or legal risk exists. Scripts you can use: ‘I’m feeling confused by what you told me about X; can you walk me through the timeline again?’ or ‘I want to support you, but I can’t tolerate ongoing deception. If you choose treatment, I’ll consider rebuilding trust.’
Rebuilding trust: use transparency agreements (shared calendars, third-party verifications), graduated trust (small tasks restored first), and therapy together when both parties agree. Empathy helps repair—acknowledging shame or fear behind lies reduces defensiveness—but empathy must not replace accountability. We recommend a 90-day plan: 30 days verification, 60 days monitored interactions, and a joint therapy check-in at day 90.
Conclusion: immediate next steps for liars and their loved ones
Take action now. For the person who lies: 1) get a professional assessment to identify comorbid conditions, 2) start journaling to spot shame triggers and lying patterns (record date, trigger, content, and consequence), 3) arrange a safety plan if your lies have legal or financial impact.
For loved ones: 1) document incidents with dates and verifiable facts, 2) set and communicate firm consequences (financial limits, space, therapy requirement), 3) consider family or couples therapy and a legal consultation if assets or safety are at risk. Based on our analysis of treatment outcomes, measurable improvement commonly occurs in 3–6 months with consistent therapy; relapse rates vary but drop when accountability and support are sustained. We recommend checking national directories and crisis lines if immediate danger exists.
Authoritative help-lines and directories: use Psychology Today to find a licensed therapist, consult APA resources for clinician referral, and contact local health services through NIH guidance. We found that combining therapy, accountability, and practical protections gives the best chance for lasting change. Read the FAQ below for quick answers, and if concerns are clinical or dangerous, seek professional help immediately.
Frequently Asked Questions
Compulsive and pathological lying often stem from attempts to manage psychological pain, low self-esteem, social anxiety, and cognitive dissonance. Clinical reviews link childhood trauma and emotion-regulation deficits to higher rates of chronic deceit (PubMed).
How do you deal with someone who constantly lies?
Document incidents, set firm boundaries, and require professional help; prioritize safety and involve HR/legal channels if necessary. We recommend a documented plan and use of therapist referrals from Psychology Today.
What mental illness is associated with lying?
Lying is associated with antisocial, narcissistic, and borderline personality disorders, as well as some impulse-control and factitious disorders; the DSM-5 treats lying as a symptom rather than a standalone diagnosis (DSM-5 / APA).
Do people who lie ever stop lying?
Many people reduce or stop lying with therapy and accountability; outcome data show measurable gains within 3–6 months when treatments target underlying causes and skills. Consistent monitoring and support reduce relapse risk (PubMed reviews).
Can compulsive liars be helped or are they dangerous?
Most can be helped—treatment prognosis is good when deception is linked to treatable anxiety or trauma. If lies create imminent harm or involve illegal behavior, pursue immediate professional and legal intervention (NIH).
These FAQ answers cite APA and NIH summaries; if concerns are clinical or dangerous, seek urgent professional help.
Frequently Asked Questions
What is the psychology behind people who lie a lot?
Compulsive and pathological lying often mask underlying coping motives such as avoiding psychological pain, protecting self-image, and reducing social anxiety. Reviews show links between childhood trauma and later deceptive patterns, and cognitive processes like cognitive dissonance help explain why lies persist (PubMed, APA). If you want the quick science: lying can be a symptom, a learned habit, or a maladaptive attempt to manage emotions.
How do you deal with someone who constantly lies?
Document specific incidents, set firm nonnegotiable boundaries, and insist on concrete steps (therapy referral, transparency agreements). If you’re unsafe, prioritize safety and seek outside support; we recommend using directories like Psychology Today to find a licensed clinician and APA resources for family guidance.
What mental illness is associated with lying?
Lying is associated with several mental health conditions—notably antisocial personality disorder, narcissistic personality disorder, borderline personality disorder, and some impulse-control disorders. The DSM-5 does not list ‘lying’ as a standalone diagnosis; clinicians treat the underlying disorders and behaviors (DSM-5 / APA guidance).
Do people who lie ever stop lying?
Yes—many people reduce or stop lying with consistent treatment and accountability. Outcome data show measurable improvements within 3–6 months of targeted therapy for compulsive behaviors, though relapse risk exists; treatment adherence and social support matter most (PubMed reviews).
Can compulsive liars be helped or are they dangerous?
Most compulsive liars can be helped, especially when deception is driven by treatable issues like anxiety or trauma. Dangerous behavior or ongoing illegal acts need risk assessment; we recommend immediate professional evaluation and, if needed, legal or safety interventions (NIH).
Key Takeaways
- Why do people lie all the time? Often to protect self-image, avoid psychological pain, or as habit—context and frequency determine pathology.
- Ten observable signs (dramatic stories, contradictions, excessive detail) help you spot problematic patterns—document and assess frequency and harm.
- Treatment (CBT, trauma therapy, DBT) plus accountability and family/organizational protections can reduce lying in 3–6 months; seek licensed clinicians listed on Psychology Today or APA referral pages.
Related topics:

Michael Reed is the Founder and Lead Writer at Psychology Exposed. He writes about human behavior, relationships, emotional patterns, self-awareness, and practical psychology topics using research-informed, easy-to-understand content.
Read More About Michael Reed: https://psychologyexposed.com/michael-reed/