
what is separation anxiety in psychology: 7 Expert Facts
what is separation anxiety in psychology: 7 expert facts on symptoms, DSM-5 diagnosis, causes, treatment and when normal worry becomes a disorder. Evidence-based next steps (2026).
Introduction — what readers are looking for
What is separation anxiety in psychology? It’s the fear, distress, or avoidance that happens when you or your child must be away from an important attachment figure, and readers usually search this because they want to know whether the reaction is normal, temporary, or a mental health disorder that needs care.
If you’re here, you likely want a straight answer. Maybe you’re a parent dealing with school refusal, a clinician reviewing DSM-5 criteria, or an adult who feels panic when a partner leaves. This is an informational piece built to explain the definition, symptoms, DSM-5 diagnosis, causes, and treatment of Separation Anxiety Disorder, with clear next steps you can actually use.
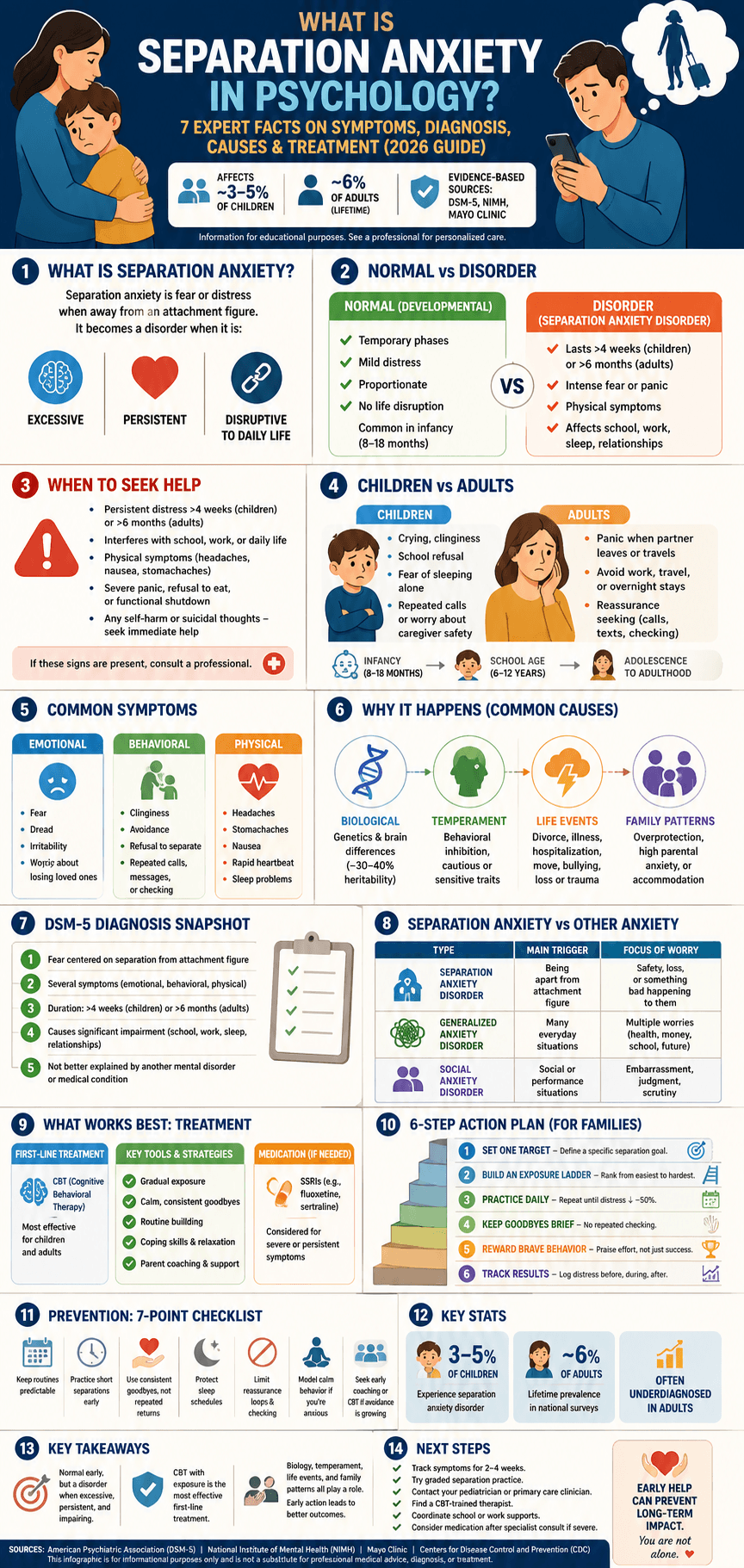
We researched current clinical sources and found that separation anxiety disorder affects roughly 3% to 5% of children in many estimates, while adult lifetime prevalence in national data is often reported around 6%. Based on our analysis of recent reviews through 2026, the condition is more common in adults than many people assume, and it can impair attendance, sleep, relationships, and work. You’ll see authoritative sources throughout, including American Psychiatric Association (DSM-5), NIMH, and Mayo Clinic.
You’ll also get a clear structure: a quick definition, differences between children and adults, common symptoms, causes including biological factors, DSM-5 diagnosis, treatment, prevention, cultural perspectives, case examples, and FAQs. That means answers to People Also Ask questions are covered as you read, including When does separation anxiety end? and How do you help someone with separation anxiety?

Quick Answer: what is separation anxiety in psychology meaning
In short, what is separation anxiety in psychology? It’s an anxiety response to real or perceived separation from an attachment figure, and it becomes a disorder when the fear is excessive for the person’s developmental stage, lasts long enough, and causes real impairment.
Use this quick checklist to tell normal developmental separation worry from a disorder:
- Duration: brief phases are common; persistent symptoms are more concerning.
- Intensity: crying at daycare drop-off is different from panic, vomiting, or daily refusal.
- Impairment: if school, sleep, work, or relationships are suffering, take it seriously.
A simple 3-step cue for when to seek help:
- Persistent distress for more than 4 weeks in children or 6 months in adults.
- Interference with daily life, such as school refusal, missed work, or inability to sleep alone.
- Physical or behavioral symptoms, such as stomachaches, headaches, tantrums, panic symptoms, or repeated checking.
These thresholds align with major medical guidance and diagnostic standards summarized by Mayo Clinic and the DSM framework used by clinicians.
what is separation anxiety in psychology — short definition
What is separation anxiety in psychology? It is excessive fear or distress about being away from a person you feel strongly attached to. In clinical settings, the DSM-5 label is Separation Anxiety Disorder, used when the fear is age-inappropriate, persistent, and disruptive to daily functioning. See APA (DSM-5).
SEO synonyms/related terms: Separation Anxiety Disorder, separation distress, separation fear.
Separation Anxiety in Children vs Adults
Separation anxiety in children often starts as a normal developmental response. During infant development, many babies show distress when a parent leaves between about 8 and 18 months. Attachment research from Bowlby and Ainsworth helped explain why: young children use an attachment figure as a base for safety. That part is normal. The issue is when fear becomes too intense for the child’s age, lasts too long, and disrupts functioning.
By school age, most children can tolerate routine separation with some support. If a 7-year-old has daily meltdowns, repeated stomachaches, or refuses school for weeks, that points beyond ordinary clinginess. Child prevalence estimates commonly land around 3% to 5%. Adults are affected too. National survey data cited in psychiatric literature have estimated adult lifetime prevalence near 6.6%, which matters because many adults are never assessed for separation-based anxiety.
Behavior looks different by age group:
- Infants and toddlers: clinginess, crying, tantrums, sleep resistance.
- School-age children: school refusal, repeated calls home, fear of sleeping alone.
- Adolescents: panic symptoms, refusal to travel or stay with peers.
- Adults: work avoidance, distress when a partner travels, repeated reassurance seeking.
The impact can be large. School refusal is linked with anxiety disorders in a substantial share of referrals, and prolonged absence can affect grades, peer relationships, and family stress. In our experience reviewing clinical patterns, adults with separation anxiety in psychology often miss shifts, avoid travel, or struggle after breakups or bereavement.
Case vignette — child: “Liam,” age 9, began refusing school after his mother had a brief hospital stay. He cried nightly, reported stomach pain most mornings, and missed 11 school days in one month.
Case vignette — adult: “Maria,” age 34, developed panic-like symptoms after a divorce. When her new partner left for work, she called repeatedly, couldn’t focus at her job, and started avoiding overnight separations.
When Separation Anxiety Becomes a Disorder
The DSM-5 does not diagnose separation anxiety just because someone dislikes goodbyes. A clinician looks for a pattern of excessive fear concerning separation from attachment figures, plus enough symptoms, enough duration, and enough impairment to qualify as an anxiety disorder. For children and adolescents, the pattern must last at least 4 weeks. For adults, it typically must last at least 6 months. The distress must also be out of proportion to the person’s developmental stage and cultural context. See APA.
Symptoms commonly include recurrent distress when separation occurs or is expected, persistent worry about losing the attachment figure, refusal to go out, refusal to sleep away, nightmares, and physical symptoms when separation happens. The final step is impairment. If there is no meaningful impact on school, social life, work, or family functioning, the threshold may not be met.
Clinicians also rule out other causes. PTSD can look similar if fear follows trauma. Generalized anxiety disorder causes broad worry, not mostly separation-based fear. Social anxiety centers on scrutiny and embarrassment. Medical causes such as gastrointestinal illness, thyroid problems, or sleep disorders can also mimic anxiety symptoms. We recommend a full clinical interview and, when needed, screening tools such as child anxiety scales or separation-specific avoidance measures.
Red flags that need faster evaluation:
- Unable to attend school or work for more than 2 weeks
- Rapid worsening after a major life event
- Severe panic, refusal to eat, or functional shutdown
- Any self-harm or suicidal thoughts — seek emergency help immediately
what is separation anxiety in psychology: DSM-5 criteria
If you want a practical screen for what is separation anxiety in psychology under DSM-5 criteria, use this 5-step checklist:
- 1. Core fear: Is the distress specifically tied to separation from an attachment figure?
- 2. Symptom count: Are there several features such as clinginess, nightmares, refusal, physical symptoms, or excessive worry?
- 3. Duration: Has it lasted over 4 weeks in children or 6 months in adults?
- 4. Impairment: Is school, work, sleep, or family life clearly affected?
- 5. Exclusion: Could another mental disorder or medical issue explain it better?
This is not a self-diagnosis tool, but it helps parents and clinicians decide when a formal evaluation is warranted.
Common Symptoms of Separation Anxiety
The symptoms of separation anxiety span emotional, behavioral, and physical systems. The emotional core is usually excessive worry about losing the attachment figure or fear that something bad will happen during separation. In children, that often sounds like “What if you die in a car crash?” In adults, it may look like repeated texting, panic before a partner’s trip, or inability to sleep alone.
Behaviorally, you may see clinginess, refusal to be alone, school refusal, sleep resistance, or repeated checking. Physiologically, symptoms often include headaches, stomachaches, nausea, sweating, palpitations, shakiness, and insomnia. Mayo Clinic and pediatric mental health sources note that somatic complaints are common in anxiety presentations, which is why children may show up first in primary care rather than therapy.
A useful way to group symptoms:
- Emotional: fear, crying, dread, irritability
- Behavioral: clinginess, tantrums, refusal to separate, repeated calls or texts
- Physiological: nausea, abdominal pain, rapid heartbeat, sleep problems
In clinic samples, somatic complaints are frequent, and some pediatric anxiety studies report them in well over 50% of anxious children. Panic-like surges may last 10 to 30 minutes, but anticipatory anxiety can last hours. Based on our analysis of symptom reports, the pattern matters more than one bad day.
To reduce observation bias, keep a simple symptom diary for 2 weeks. Record the time, trigger, what the person feared, intensity from 1 to 10, physical symptoms, and what happened after reassurance or avoidance. This gives clinicians better data than memory alone. See CDC and Mayo Clinic.
Causes of Separation Anxiety
There is no single cause. What drives separation anxiety in psychology is usually a mix of developmental, environmental, and biological factors. Some children are temperamentally more cautious from infancy. Others develop symptoms after a stressor such as divorce, moving, hospitalization, bullying, or the death of a loved one. Adults may first show the disorder after a breakup, childbirth, illness, or sudden loss of safety.
The biological side deserves more attention than most articles give it. Twin and family studies suggest a moderate heritable component to childhood anxiety disorders, often in the range of roughly 30% to 40% depending on the sample. Neuroimaging research from 2020 to 2024 has also linked anxiety vulnerability to altered threat processing in brain regions such as the amygdala and prefrontal circuits. NIMH-backed research on anxiety broadly supports the idea that fear circuits can become overreactive in susceptible people.
Temperament matters too. Behavioral inhibition—a tendency to withdraw from new people or situations—raises later anxiety risk. Add a traumatic separation or highly anxious caregiving, and the risk climbs further. Example: a cautious child who already hates novelty may develop full Separation Anxiety Disorder after being left unexpectedly in the hospital for several days.
Cultural context changes both presentation and help-seeking. In more collectivist settings, close family dependence may be more accepted, which can delay recognition of impairment. In more individualist cultures, the same behavior may be labeled a problem earlier. We found that stigma, language barriers, and parental anxiety are modifiable barriers clinicians should screen for. Helpful targets include sleep routines, predictable departures, parental modeling, and reducing excessive accommodation.
Separation Anxiety vs General Anxiety
Many families ask whether the problem is really separation anxiety or a broader anxiety disorder. The simplest answer is to look at the focus of the fear. If the worry spikes mainly when the person is away from an attachment figure, that points toward separation anxiety. If the person worries about grades, health, disasters, money, and many daily topics, generalized anxiety disorder may fit better. If fear centers on embarrassment or social judgment, social anxiety is more likely.
Quick comparison:
| Condition | Main trigger | Focus of worry | Common pattern |
| Separation Anxiety Disorder | Being apart | Safety/loss of attachment figure | Clinginess, school refusal, sleep refusal |
| Generalized Anxiety Disorder | Many situations | Multiple everyday worries | Chronic “what if” thinking |
| Social Anxiety Disorder | Social exposure | Embarrassment, scrutiny | Avoiding speaking, performance, peers |
Comorbidity is common. Anxiety disorders often overlap with depression, specific phobias, and GAD, which is one reason accurate diagnosis matters. A practical rule of thumb for normal worry: it is proportionate to the stressor, short-lived, and not impairing. A child who cries for 5 minutes at camp drop-off but settles quickly is different from a child who vomits nightly and misses school for weeks.
When sorting this out, ask three questions: Where is the worry focused? What triggers it? What does the person avoid? Those answers often clarify the diagnosis faster than labels alone.
How It Is Treated
The first-line treatment for separation anxiety is usually psychological treatment, especially cognitive behavioral therapy (CBT) and related behavioral therapy methods. Across child anxiety trials, CBT has shown meaningful benefits, and treatment guidelines consistently place it ahead of medication for mild to moderate cases. For severe, persistent, or comorbid cases, clinicians may add an SSRI such as fluoxetine or sertraline, but medication is usually second-line and requires monitoring. See NIMH and FDA.
6-step parent-focused behavioral plan:
- Set one target: define a specific separation goal, such as 10 minutes with grandma or one full school drop-off.
- Build an exposure ladder: rank separations from easiest to hardest.
- Practice daily: repeat small separations until distress drops by about 50%.
- Use brief, calm goodbyes: no repeated checking or sneaking out.
- Reward brave behavior: praise effort, not just success.
- Track results: log distress before, during, and after each practice.
Therapy should match age. Preschoolers may benefit from play-based CBT with parent coaching. School-age children usually do well with standard CBT and exposure. Adults may need CBT focused on attachment beliefs, panic management, and relationship patterns, sometimes with medication if symptoms are severe. For the common question, what is the best therapy for separation anxiety in children? The strongest answer is CBT plus parent training.
Schools and employers matter too. Helpful supports include phased returns, reduced check-ins that are planned rather than constant, 504 plans where appropriate, and school-based CBT coordination. Teletherapy has also improved access. Studies from 2020 to 2025 suggest tele-CBT can be effective for many anxiety disorders when exposure work is built in. Consider intensive outpatient or inpatient care if functioning collapses, risk rises, or outpatient treatment fails.
Parent-Child Relationship, Long-Term Outcomes, and Prevention
One of the biggest hidden drivers of separation anxiety is the parent-child relationship pattern around fear. Parents often try to reduce distress by staying longer, allowing school avoidance, sleeping with the child, or offering repeated reassurance. It makes sense in the moment, but this type of accommodation can maintain the cycle. Research in pediatric anxiety has found high accommodation rates in families, often well above 60% in clinical samples.
Untreated separation anxiety can have real long-term effects. Longitudinal studies suggest that childhood anxiety disorders raise later risk for adult anxiety, depressive symptoms, and social or work impairment. In plain terms, the disorder can follow you forward if no one interrupts the avoidance pattern. Based on our analysis of follow-up studies, early treatment is linked to better school attendance, less family conflict, and lower ongoing impairment at 6- to 12-month follow-up.
7-point prevention checklist:
- Keep routines predictable
- Practice short, calm separations from early childhood
- Use consistent goodbyes, not repeated returns
- Protect sleep schedules
- Limit reassurance loops and excessive checking
- Model calm behavior if you are anxious yourself
- Seek early parent coaching or CBT if avoidance starts growing
For clinicians, family-based interventions are often essential. Include parent training when accommodation is high, when school refusal is present, or when parental anxiety is reinforcing symptoms. Prevention is not perfect, but it meaningfully lowers risk and speeds recovery when symptoms are caught early.
Cultural Perspectives, Case Studies, and Real-World Examples
Cultural norms shape what counts as acceptable dependence, how quickly families seek help, and how symptoms are described. In some Mediterranean or Latin family systems, close interdependence may be expected longer into adolescence. In many Northern European settings, independence is encouraged earlier. Neither is automatically right or wrong. The clinical question is whether the fear causes impairment in that person’s real environment.
Case study 1 — school-aged child: An 8-year-old girl developed school refusal after her father changed jobs and started traveling weekly. Over 6 weeks, CBT plus parent coaching built a morning exposure plan, reduced reassurance, and coordinated a phased school return. By week 8, attendance improved from 2 days per week to 5, and morning distress ratings fell from 9/10 to 4/10.
Case study 2 — adult: A 39-year-old man developed separation anxiety after divorce and a health scare. He had nightly panic, called his partner repeatedly, and avoided overnight work trips. Over 12 weeks, adult CBT and sertraline reduced panic frequency, and he completed two work trips with manageable anxiety. Functional improvement, not just symptom relief, was the key marker.
A composite testimonial-style summary sounds like this: “I thought I was just a worried parent. Then I realized my own fear was making drop-offs harder. Once we stuck to one goodbye and a step plan, mornings changed.” If you use real quotes in practice, anonymize them and get permission.
Helpful resources: NIMH, WHO, and NHS. Clinicians can adapt care by translating handouts, involving trusted community leaders, and checking whether cultural values about closeness are being mistaken for pathology.
Conclusion: Next Steps If You’re Worried
If you’re worried about separation anxiety, focus on what you can measure and change this week. We found that the best next steps are usually practical, not dramatic.
- Track symptoms for 2 to 4 weeks.
- Try graded separation practice at home.
- Contact your pediatrician or primary care clinician.
- Find a CBT-trained therapist with child anxiety or adult anxiety experience.
- Consider medication only after a specialist consult if symptoms are severe.
- Coordinate school or work supports, such as phased returns or planned accommodations.
Based on our analysis, separation anxiety improves most when avoidance is addressed early and consistently. We found that waiting for it to “just pass” often prolongs the cycle, especially when school refusal, panic, or repeated accommodation are already present. For evidence-based next steps, start with APA, NIMH, and Mayo Clinic.
As of 2026, telehealth has made it easier to get specialty care even if you live far from a pediatric anxiety clinic. Search clinician directories, ask your pediatrician for referrals, or use reputable telehealth platforms. A strong first search term is: “child CBT for separation anxiety near me”. That one step can turn vague worry into a real treatment plan.
Frequently Asked Questions
These are short, direct answers to the most common follow-up questions readers ask after learning what is separation anxiety in psychology.
When does separation anxiety end?
Typical developmental separation worries often peak between about 9 and 18 months and ease as children mature, with many improving by school age. We researched age-trajectory guidance and found that if intense symptoms continue past the expected developmental stage, or last more than 4 weeks in children or 6 months in adults, referral is appropriate. See Mayo Clinic.
How do you help someone with separation anxiety?
Help starts with calm validation, predictable routines, and graded exposure rather than repeated rescue. CBT is the best-supported treatment approach, and many studies show meaningful symptom reduction when exposure work is done consistently. Immediate steps: make a short separation plan, keep goodbyes brief, reward brave behavior, and seek professional care if school or work is affected. See NIMH.
What is the best therapy for separation anxiety in children?
The best therapy for most children is cognitive behavioral therapy with parent involvement. Reviews of child anxiety treatment consistently support CBT as first-line care because it directly targets avoidance, distorted fear, and coping skills. To find the right clinician, look for training in child CBT, exposure-based treatment, and parent coaching.
Which dog breed has the worst separation anxiety?
No single breed universally has the worst separation anxiety, but veterinary behavior data often report higher rates in breeds such as Labrador Retrievers, German Shepherds, Border Collies, and some companion breeds. This is a canine behavior issue, not the same as human Separation Anxiety Disorder. For dogs, gradual alone-time training, exercise, and enrichment are the usual first steps.
Can separation anxiety be prevented?
Sometimes, especially when you act early. Consistent routines, gradual separation practice from infancy, calm parental behavior, and early coaching for anxious families can reduce risk. Some early intervention programs have shown lower later anxiety symptoms, though prevention is not guaranteed for every child.
Frequently Asked Questions
When does separation anxiety end?
Typical developmental separation worries often peak between about 9 and 18 months and ease as children gain confidence, with many improving by early school age. We researched pediatric guidance and found that when symptoms stay intense past the expected developmental stage, last more than 4 weeks in children or 6 months in adults, or disrupt school, sleep, or work, it’s time to seek professional help from a pediatrician or mental health clinician. See Mayo Clinic and APA.
How do you help someone with separation anxiety?
Start with validation, then use graded exposure, predictable routines, and calm goodbyes instead of repeated reassurance. CBT helps many people significantly; based on our analysis of treatment reviews, structured CBT with parent or family involvement is the best-supported first step, especially when symptoms interfere with school or work. A quick checklist: name the fear, plan one small separation practice, track distress from 1 to 10, and contact a clinician if avoidance is growing. See NIMH and Mayo Clinic.
What is the best therapy for separation anxiety in children?
The best-supported therapy for children is cognitive behavioral therapy (CBT) with parental involvement. Trials and reviews consistently show that exposure-based CBT reduces avoidance, physical symptoms, and school refusal better than reassurance alone, and parent training improves follow-through at home. Practical tip: look for a therapist trained in child anxiety, exposure work, and parent coaching.
Which dog breed has the worst separation anxiety?
There isn’t one single breed with the “worst” separation anxiety, but studies and veterinary behavior reports often flag Labrador Retrievers, German Shepherds, Border Collies, Cocker Spaniels, and some small companion breeds as higher-risk groups. That said, canine separation anxiety depends as much on temperament, early training, routine changes, and owner absence patterns as on breed. This differs from human Separation Anxiety Disorder; for dogs, use gradual alone-time training, enrichment, and ask a veterinarian or veterinary behaviorist for help.
Can separation anxiety be prevented?
Sometimes, yes. Consistent caregiving routines, short planned separations, calm goodbyes, and early parent coaching can lower risk, especially in children with behavioral inhibition or anxious parents. We found early intervention matters: family-based anxiety programs have shown measurable reductions in later anxiety symptoms at follow-up, though they don’t prevent every case. If your child is already avoiding school or can’t separate without major distress, prevention shifts to early treatment.
Key Takeaways
- Separation anxiety is normal in early development, but it becomes a disorder when it is excessive, persistent, and clearly impairs school, work, sleep, or relationships.
- The strongest first-line treatment is CBT with exposure, often paired with parent training for children and sometimes SSRIs for severe cases.
- Biology, temperament, stressful life events, and family accommodation all shape risk, so treatment works best when it addresses both the person and the environment.
- Early action matters: track symptoms, reduce avoidance, involve school or work supports, and seek a clinician if symptoms last beyond DSM-5 thresholds or worsen quickly.

Michael Reed is the Founder and Lead Writer at Psychology Exposed. He writes about human behavior, relationships, emotional patterns, self-awareness, and practical psychology topics using research-informed, easy-to-understand content.
Read More About Michael Reed: https://psychologyexposed.com/michael-reed/