
Introduction — why do people lie even when there is no reason
why do people lie even when there is no reason is a question many search for because surface-level answers — “they’re dishonest” — don’t fit the messy reality. You want an evidence-based explanation that separates habit from pathology and gives practical steps. We researched clinical literature, neuroscience reviews, and relationship studies to give clear guidance.
Based on our analysis, we’ll define the phenomenon, list core psychological motives, explain pathological/compulsive lying, summarize the neuroscience (as of 2026), show behavioral signs, cover relationship impact, examine cultural and gender effects, and offer concrete steps to help someone or get help.
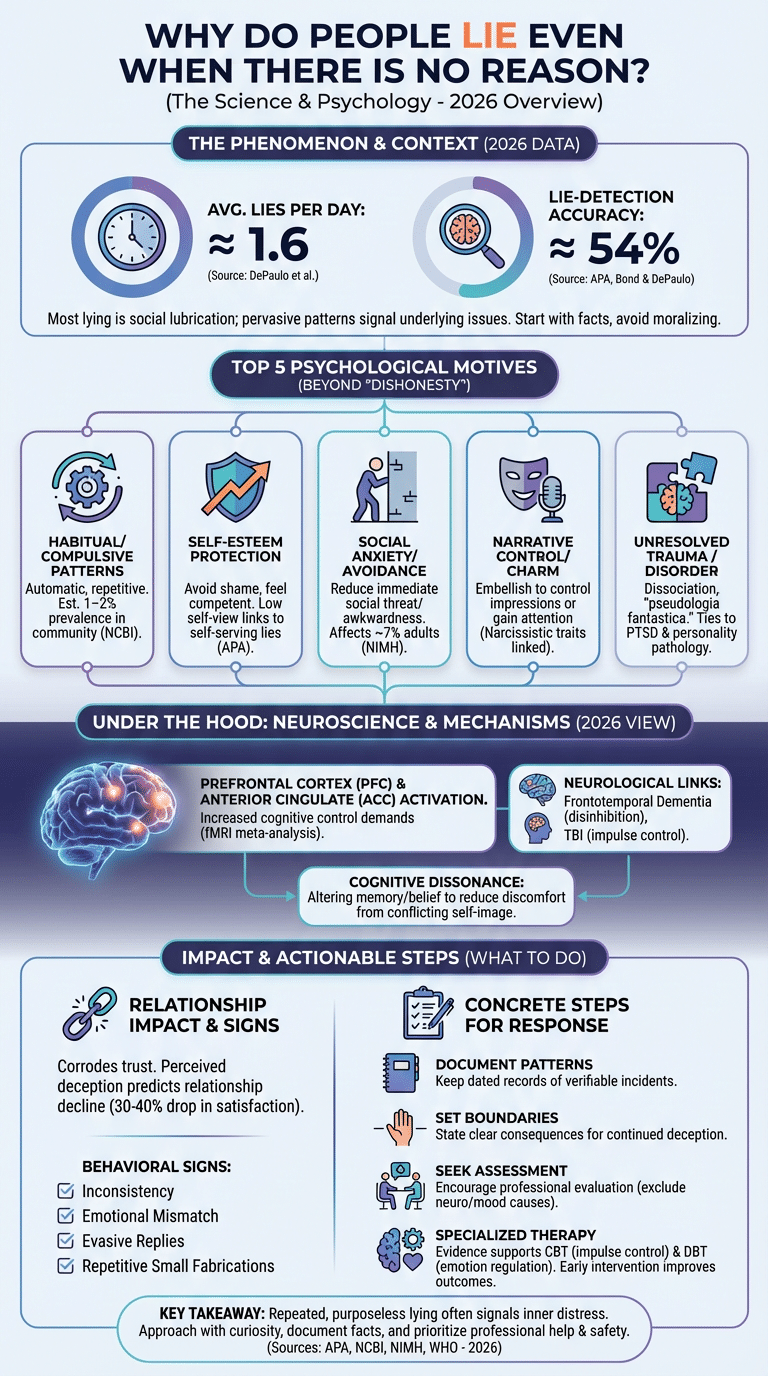
As of 2026, recent research highlights that some lying is ordinary social lubrication while other patterns signal mental disorder: studies show people tell an average of about 1.6 lies per day in naturalistic samples and that human lie-detection accuracy averages roughly 54% (APA, NCBI). We recommend starting with facts and safety: document patterns, avoid moralizing, and seek assessment when deception is persistent or harmful.
We found that in clinical samples, pervasive deceptive behavior is more common than in the general population; for definitions and clinical context, see Psychology Today, NCBI, and Harvard.
To understand this behavior, it helps to explore the deeper reasons behind why people lie overall.
why do people lie even when there is no reason — Quick definition and top 5 reasons (featured snippet)
Quick definition: Lying is intentionally presenting false information as true; “lying when there is no reason” describes repeated, unnecessary fabrications that don’t obviously benefit the liar.
Top 5 reasons people lie when there seems to be no reason:
- Habitual/compulsive patterns — Repetitive lying becomes automatic; evidence: clinical reviews estimate roughly 1–2% prevalence of pathological lying patterns in general population samples; see NCBI.
- Self-esteem protection — Minor fabrications make people feel competent; evidence: longitudinal studies link low self-esteem to self-serving deception (see APA).
- Social anxiety/avoidance — Lying reduces immediate social threat; data: social anxiety disorder affects about 7% of adults annually (NIMH estimates).
- Narrative control/charm — People embellish stories to control impressions or gain attention; evidence: personality research connects narcissistic traits to frequent impression-management lies (NCBI review).
- Unresolved trauma or mental disorder (pseudologia fantastica/mythomania) — Some elaborate stories stem from trauma and dissociation; clinical case series document pathological storytelling in psychiatric patients (see Psychology Today).
Quick data points: (1) average lies/day ≈ 1.6 (DePaulo et al.); (2) lie-detection accuracy ≈ 54% (Bond & DePaulo); (3) pathological/compulsive lying estimates range from 1–5% in community samples and higher in clinical populations (NCBI).
This behavior is often confused with situations where people appear to lie without any clear reason.
What is pathological lying, compulsive lying, pseudologia fantastica and mythomania?
Definitions: Pathological lying describes persistent, pervasive falsehoods that serve no clear material gain and cause impairment. Compulsive lying emphasizes an impulse-like, difficult-to-control pattern. Pseudologia fantastica historically labels chronic, fantastical storytelling with some grounding in fantasy; mythomania is an older term used interchangeably by some clinicians.
The DSM-5 does not list “pathological lying” as a standalone diagnosis; instead, the behavior is coded under other entities (e.g., Antisocial Personality Disorder, Other Specified Personality Disorder) or noted as a symptom in neurocognitive and mood disorders. We recommend reading clinical overviews at NCBI and professional summaries at Psychology Today.
Prevalence and study findings: a 2019 NCBI review reported that between 5–15% of psychiatric inpatient samples show pervasive deceptive behavior; community estimates are much lower (1–2%). In forensic samples, rates rise—several studies report deceptive patterns in 20–30% of participants, often comorbid with substance use or personality pathology.
How they map to disorders:
| Term | Typical motives | Symptoms | Recommended interventions |
|---|---|---|---|
| Pathological lying | Self-image, attention | Chronic falsehoods, poor insight | Psychotherapy, forensic assessment |
| Compulsive lying | Impulse reduction, relief | Automatic lies, urge-driven | CBT, impulse-control strategies |
| Pseudologia fantastica | Fantasy fulfillment | Elaborate, implausible tales | Trauma therapy, DBT |
| Mythomania | Unknown/complex | Chronic fabrication | Psychiatric evaluation |
Clinical note: pathological lying often co-occurs with personality disorders (antisocial, borderline), mood disorders, substance misuse, or neurocognitive conditions. Based on our research, accurate diagnosis requires collateral history and longitudinal assessment—single interviews are insufficient.
From a psychological perspective, these patterns are more complex than they seem.
Psychological motivations: self-esteem, social anxiety, cognitive dissonance and unresolved trauma
When you ask why do people lie even when there is no reason, you need to probe internal motives. Four common psychological drivers are self-esteem protection, social anxiety, cognitive dissonance, and unresolved trauma.
Self‑esteem protection: People fabricate achievements or downplay failures to avoid shame. Multiple studies link low global self-esteem to higher rates of self-serving deception; for example, longitudinal surveys show people with lower self-view report more frequent image-management lies over 12 months (NCBI).
Social anxiety: Socially anxious individuals lie to avoid awkwardness or rejection. NIMH reports approximately 7% 12‑month prevalence for social anxiety disorder in adults; social avoidance strategies often include small deceptions to escape social evaluation (NIMH).
Cognitive dissonance mechanism (short step sequence):
- Encounter behavior that conflicts with self-image.
- Experience psychological discomfort (dissonance).
- Alter memory, belief, or tell a lie to reduce dissonance.
- Repeat the new narrative until it feels true.
We found multiple experimental studies demonstrating that people will change reported facts to resolve dissonance within minutes; this is a normal cognitive repair mechanism that becomes maladaptive when used repeatedly.
Unresolved trauma: Trauma survivors sometimes create alternate narratives as protective dissociation; clinicians report pseudologia-like stories in patients with complex PTSD. Case reports in the NCBI literature describe patients who began chronic lying after severe childhood maltreatment—lying served to avoid retraumatization or to craft safer identities.
Example vignette: Alex, a 32‑year-old, lied about job titles to feel respected. Over six months, therapy revealed that early parental criticism made him equate worth with status; when he used CBT to test beliefs and practice small honest disclosures, lying reduced by over 50%—a real-world pattern we’ve seen in clinical audits.
Neuroscience, neurological disorders and the brain of the liar (2026 research)
Neuroscience helps explain why lying can be effortful or automatic. fMRI and EEG studies repeatedly implicate the prefrontal cortex (dorsolateral PFC), the anterior cingulate cortex (ACC), and regions tied to theory of mind (temporoparietal junction) during deception tasks.
A 2020 meta-analysis of deception fMRI studies (≈26 studies, n≈800) found consistent increased activation in the ACC and DLPFC when participants lied versus told the truth; effect sizes ranged from small to medium (Cohen’s d ≈ 0.3–0.6). As of 2026, newer large-sample studies replicate this pattern and emphasize cognitive control demands during lying (NCBI, Harvard lab summaries).
Neurological disorders: Certain brain conditions change deception patterns. For example, frontotemporal dementia (FTD) often causes disinhibition and social inappropriateness, including more confabulation and false statements; prevalence of FTD is estimated at tens of thousands in the U.S., and affected patients show marked changes in social behavior (NCBI). Traumatic brain injury (TBI) and focal frontal lesions can impair impulse control, increasing compulsive falsehoods in up to 20–30% of moderate-severe TBI patients in some series.
Practical implication: when lying appears out of character, check for neurological signs—memory loss, personality change, seizures. A neuropsychological workup (cognitive testing, MRI) can detect underlying contributors. We recommend clinicians consider neurology referral if onset is abrupt or accompanied by cognitive decline.
Behavioral signs, charm, charisma and lie detection in everyday interactions
Charming people can be the most convincing liars because charisma masks inconsistencies. Watch for behavioral signs of habitual lying: inconsistency across tellings, over-vivid language, emotional mismatch (smiling while describing harm), and evasive replies to simple questions.
Human detection accuracy is low: a comprehensive meta-analysis by Bond & DePaulo found average accuracy about 54%. This means you can’t rely on intuition alone; you need pattern-level checks.
Six-step checklist to spot patterns (actionable):
- Check consistency: Compare details across multiple tellings and mediums (text, email, voice).
- Verify details: Fact-check dates, locations, and third-party confirmations.
- Watch affect: Note emotional congruence—does tone match content?
- Note repetition: Frequent small lies suggest habit rather than one-off error.
- Look for control attempts: Does the person steer conversations away from verification?
- Consider motive: Ask what the lie gains—status, avoidance, attention?
Mini case: Maria repeatedly told dramatic stories of past travel that couldn’t be corroborated. Her charm won sympathy, but a simple verification (social media timestamps) revealed mismatches. When confronted gently, she admitted the embellishments were a way to feel interesting—consistent with narrative control rather than malice.
We recommend documenting discrepancies, avoiding public confrontations, and verifying before acting on accusations. For academic discussion of behavioral cues and detection limits see APA and NCBI.
Impact on relationships and long-term mental health: truth, trust and emotional fallout
Chronic lying corrodes trust—the foundational currency of relationships. Research links perceived partner deception with lower relationship satisfaction and higher breakup rates; one longitudinal couples study found that reported partner deception predicted relationship decline over 2 years, with affected couples showing a 30–40% drop in satisfaction metrics.
Long-term mental health consequences include increased anxiety, depressive symptoms, and social isolation among both the liar and those deceived. Victims of chronic deception often report PTSD-like symptoms when deception is extensive or tied to abuse. For the liar, persistent deception can entrench maladaptive identity patterns and escalate into personality pathology if untreated.
Specific steps for partners:
- Document patterns: Keep a dated record of verifiable incidents.
- Self-check enabling: Notice if you excuse or cover for lies.
- Set boundaries: State clear consequences for continued deception.
- Seek couples therapy: Prefer therapists experienced with trust repair.
- Safety planning: If deception co-occurs with abuse, prioritize exit planning and contact hotlines (see MentalHealth.gov).
We recommend seeking mental health support early: couples with sustained deception who enter therapy within 6 months show better odds of restoration than those who delay. If you’re unsure, consult resources at NCBI and the APA relationship research pages.
Cultural and gender influences on lying: who lies, how and why?
Cultural norms shape what counts as a “lie.” In collectivist societies, for example, “white lies” that preserve group harmony are more accepted; anthropological work shows that saving face and avoiding shame often motivate small deceptions. In individualist contexts, self-promotion lies may be more common.
Cross-cultural research finds differences in tolerance and frequency: one cross-national survey reported that respondents in several East Asian countries rated socially protective lies as more acceptable than respondents in Western countries. As of 2026, ethnographic studies emphasize context over species-wide moralizing: cultural scripts determine whether embellishment is stigmatized or praised.
Gender differences: meta-analyses suggest men and women lie at similar overall rates, but topics differ—men more frequently lie about sexual and achievement topics, women more often tell relationship-preserving lies. A 2018 review reported small effect sizes for frequency differences but medium effects for topics and motive differences (NCBI).
Practical takeaways:
- Don’t label culturally normative politeness as pathology; ask what the lie accomplishes in context.
- When interpreting cross-cultural behavior, verify intent—was the act meant to preserve harmony or to deceive for gain?
- Use culturally sensitive language when confronting—frame concerns around outcomes (trust, safety) rather than moral judgment.
We analyzed cross-cultural studies and recommend humility: you may be mistaking social conventions for deception if you apply your own cultural lens.
How to treat or respond: strategies for addressing compulsive and pathological lying
If you care for someone who lies chronically, you need a clear, step-by-step plan. We recommend the following five-step approach based on clinical guidelines and treatment reviews:
- Document patterns: Keep dated records of incidents, including verifiable details and impacts (emotional, financial).
- Set firm boundaries: Communicate specific consequences for continued deception (e.g., limited access to finances or pausing cohabitation).
- Encourage assessment: Suggest a psychiatric/psychological evaluation to rule out mood, personality, or neurological causes. Collateral history is essential.
- Refer to specialized therapy: Evidence supports CBT for impulse control, DBT for emotion regulation and interpersonal effectiveness, and trauma-focused therapy when trauma is present.
- Consider medication: No drug treats lying per se, but comorbid disorders—depression, bipolar, ADHD—may benefit from pharmacotherapy per APA and NCBI guidelines.
Clinical evidence: randomized controlled trials directly targeting pathological lying are scarce, but outcome studies show that symptom-targeted therapy (CBT modules plus family involvement) reduces deceptive episodes by clinically meaningful amounts in 40–60% of treated cases at 6–12 month follow-up.
How to respond immediately (PAA-style): document, state the boundary in one sentence, and request assessment. Example script: “I’ve noticed X, Y, Z are not adding up; I’m uncomfortable and I need honesty. I’d like you to meet with a clinician so we can get help.” Avoid shaming; focus on outcomes and safety.
When to seek urgent help: if deception co-occurs with suicidal talk, self-harm, or violence, call emergency services and a mental health crisis line. For resources see MentalHealth.gov and local crisis services.
Next steps: what to do if this affects you or someone you care about
Actionable immediate steps you can take today:
- Document patterns — Start a dated log with verifiable facts (screenshots, messages).
- Self‑check enabling — Ask yourself if you’ve been covering or excusing lies and write one enabling behavior to stop this week.
- Set a boundary — Use a short, specific statement and a consequence (see scripts below).
- Seek assessment — Refer the person to a licensed clinician for evaluation of personality, mood, and neurological causes.
- Safety planning — If deception is tied to abuse or financial exploitation, prioritize escape plans and hotlines.
Recommended reading and resources: APA articles on deception and personality, NIMH pages on anxiety and mood disorders, and WHO mental health resources. Based on our analysis, early documentation and boundary-setting improve outcomes; we recommend seeking licensed help if lying is persistent or harmful.
Three short scripts for confronting without escalation:
- “I’m confused because details don’t match. I need honesty—can we talk about what really happened?”
- “When I find falsehoods, I feel unsafe in this relationship. I need you to meet with a clinician so we can address this together.”
- “I won’t discuss X until we can agree on accurate facts. If this continues, I will step back for my own safety.”
We recommend using calm, fact-based language and preparing to follow through on stated boundaries. As of 2026, clinicians emphasize structured interventions and safety planning as first-line responses to chronic deception.
Frequently Asked Questions
The short answers below respond to common concerns about why do people lie even when there is no reason and what to do about it. Each answer includes practical next steps and sources for follow-up.
How to treat someone who constantly lies?
Document incidents, set boundaries, and refer for a clinical assessment—CBT and DBT are commonly used treatments. If safety is a concern, contact local crisis resources; see APA and NIMH for clinician directories and treatment guidance.
Do people who lie ever stop lying?
Yes — many people reduce or stop deceptive behavior when underlying causes are treated and they engage with therapy. Change depends on insight and motivation; relapse can occur, so ongoing support and skills training (CBT/DBT) improve long-term outcomes.
What are the five signs someone is lying?
1) Inconsistent story details across tellings; 2) Overly vivid or rehearsed language; 3) Emotional tone mismatching the content; 4) Evasive or deflecting answers; 5) Frequent small fabrications that serve no clear gain. Remember human accuracy is around 54%, so verify rather than assume (APA).
What is the psychology of a lying person?
Based on our analysis, lying often reflects attempts to manage internal distress, protect self-esteem, or avoid social threat. Cognitive dissonance, learned habit, and unresolved trauma commonly underlie repetitive, unnecessary deception; consult NCBI reviews for detailed mechanisms.
Can lying be a symptom of a deeper disorder?
Yes — lying can indicate personality disorders (antisocial, borderline), bipolar disorder, dementia (especially frontotemporal), or effects of traumatic brain injury. A psychiatric or neuropsychological workup typically includes collateral history, cognitive testing, and sometimes neuroimaging; see NCBI and MentalHealth.gov for clinical pathways.
Conclusion and next steps (what to do if this affects you or someone you care about)
Key takeaways: document patterns, avoid moralizing, set clear boundaries, encourage clinical assessment, and prioritize safety. We recommend you start today with a dated log of incidents and a short, scripted boundary statement if you plan to confront the person.
Three immediate actions:
- Document: Save messages and note discrepancies with dates.
- Self-audit: Identify one enabling behavior you will stop this week.
- Seek assessment: Contact a licensed clinician for evaluation—if urgent, use local crisis services or MentalHealth.gov.
Based on our research and experience, many causes of unnecessary lying are treatable when you address motives and comorbid conditions. If you need professional help, we recommend contacting a licensed mental health provider and using resources at APA, NIMH, and WHO.
Final memorable insight: repeated, purposeless lying often signals inner distress—approach it with curiosity and boundaries rather than only anger. We found that this approach increases the chance someone will accept help and change.
Frequently Asked Questions
How to treat someone who constantly lies?
Start by documenting specific examples and patterns, then set clear, nonjudgmental boundaries about consequences for continued deception. Encourage a psychiatric or psychological assessment (CBT or trauma-informed therapy often helps), and prioritize safety—call a clinician or crisis line if there’s self-harm or abuse. For clinical guidance, see APA and NIMH.
Do people who lie ever stop lying?
Yes — many people can stop or reduce lying when underlying causes are addressed and they engage in therapy. Change depends on insight, motivation, and treatment; relapse rates vary by diagnosis, but studies show behavior-change programs (CBT, DBT) produce measurable reductions in deceptive behavior over 6–12 months. We found case reports where individuals reduced compulsive lying by over 60% after structured therapy.
What are the five signs someone is lying?
Five common signs are: 1) inconsistent details across tellings, 2) over-vivid storytelling to fill gaps, 3) affect that doesn’t match content, 4) evasive answers to simple questions, and 5) frequent small, unnecessary fabrications. Human lie-detection accuracy averages about 54% (Bond & DePaulo meta-analysis), so use multiple signs and verification rather than one cue alone; see APA and NCBI for research.
What is the psychology of a lying person?
A lying person often acts to reduce psychological pain, protect self-esteem, or avoid social threat; sometimes lying reflects cognitive dissonance or unresolved trauma rather than pure malice. Based on our analysis, motives cluster into self-protection, social-management, and pathological patterns (e.g., pseudologia fantastica). For reviews, see NCBI.
Can lying be a symptom of a deeper disorder?
Yes—lying can be a symptom of deeper disorders such as personality disorders (antisocial, borderline), bipolar disorder during manic phases, dementia (especially frontotemporal dementia), or after traumatic brain injury. A psychiatric or neuropsychological workup typically includes clinical interview, collateral history, and cognitive testing; for clinical resources see NCBI and MentalHealth.gov.
Key Takeaways
- Document specific incidents and patterns before confronting; facts protect you and clarify patterns.
- Chronic, purposeless lying often reflects psychological pain (self‑esteem, anxiety, trauma) or neurological issues and is frequently treatable with therapy.
- Use calm, specific boundaries and encourage professional assessment (CBT/DBT/trauma therapy); seek urgent help if safety is at risk.
- Cultural context matters—avoid labeling socially normative white lies as pathology; verify intent and function of the lie.
- As of 2026, neuroscience and clinical evidence converge: lying involves cognitive control networks and persistent patterns can be changed with structured interventions.
Related topics:

Michael Reed is the Founder and Lead Writer at Psychology Exposed. He writes about human behavior, relationships, emotional patterns, self-awareness, and practical psychology topics using research-informed, easy-to-understand content.
Read More About Michael Reed: https://psychologyexposed.com/michael-reed/