
Behavioral psychology principles explain how actions become more likely, less likely, automatic, avoided, repeated, or replaced. They are useful because many everyday behaviors are not shaped by insight alone. People also learn from timing, cues, consequences, comfort, discomfort, rewards, social responses, and what becomes easier with repetition.
This does not mean people are simple machines. Thoughts, emotions, biology, relationships, culture, and personal values all matter. Behavioral psychology simply gives us a practical lens for one part of human behavior: what people learn to do based on what happens before and after an action.
These principles show up in classrooms, workplaces, parenting, fitness, spending, digital habits, anxiety avoidance, procrastination, and relationship routines. Used responsibly, they help people understand behavior without shame. Used carelessly, they can become controlling, so ethics matter as much as technique.
Quick Answer
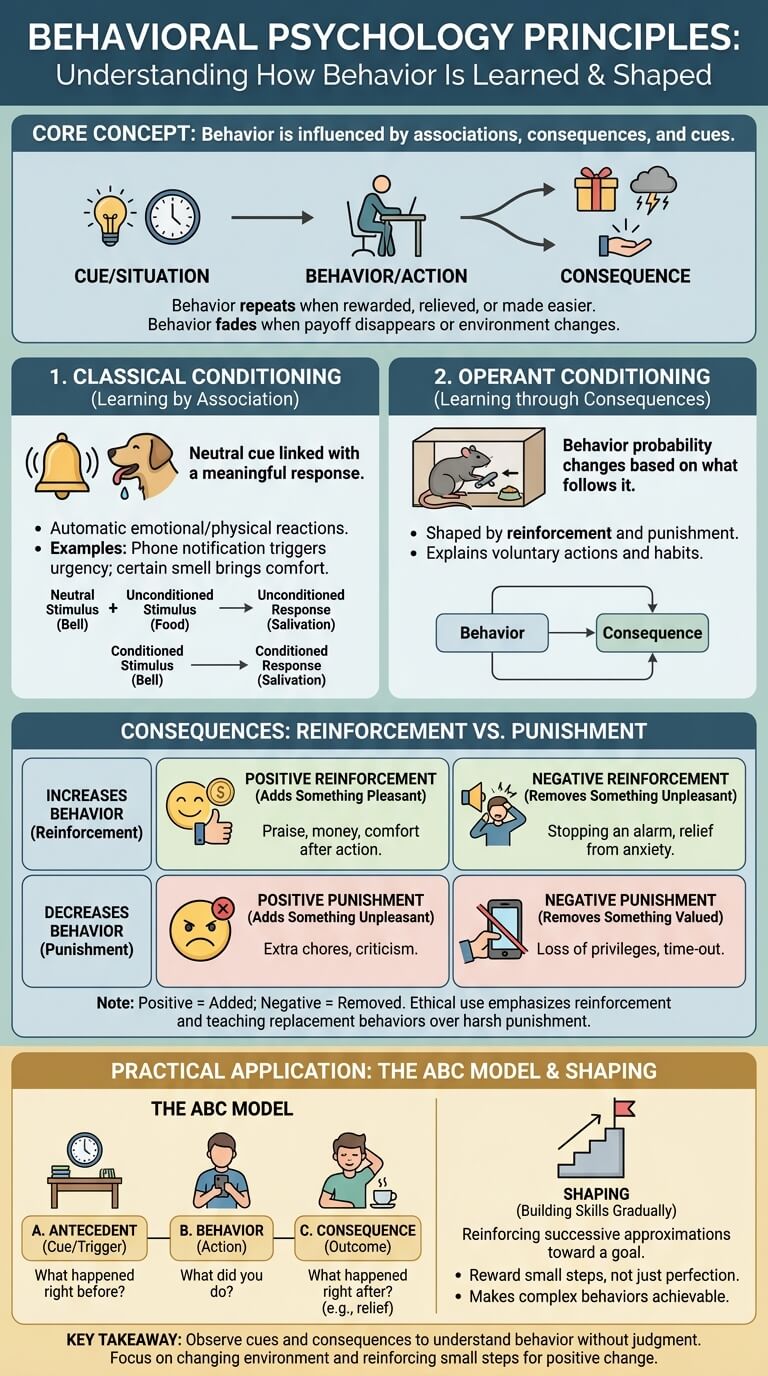
Behavioral psychology principles are ideas about how behavior is learned and shaped through association, consequences, cues, reinforcement, punishment, and gradual practice. The core lesson is simple: behavior often repeats when it is rewarded, relieved, made easier, or consistently followed by a useful outcome. Behavior often fades when the payoff disappears, the environment changes, or a better replacement behavior is learned.
What Behavioral Psychology Studies

Behavioral psychology studies observable behavior and the learning conditions that influence it. Instead of starting with hidden motives, it asks: what happened before the behavior, what did the person do, and what happened afterward? These principles sit inside the broader study of behavior.
The APA Dictionary of Psychology describes behaviorism as an approach that emphasizes observable behavior and the role of learning. Modern psychology is broader than behaviorism alone, but behavior-based explanations are still helpful because they focus on patterns that can be noticed and adjusted.
Observable behavior, learning, consequences, and context
An observable behavior is something a person does that another person could see, hear, measure, or describe. Examples include checking a phone, raising a hand, avoiding a task, apologizing, yelling, exercising, arriving late, or asking a question.
Behavioral psychology pays attention to four practical questions:
- What cue or situation tends to come before the action?
- What does the person actually do?
- What happens right after the behavior?
- Does that result make the behavior more or less likely next time?
For example, a person may check their phone whenever they feel bored. The cue is boredom, the behavior is checking, and the consequence is quick stimulation. If that stimulation feels rewarding, the checking becomes more likely the next time boredom appears.
Why behaviorism still matters today
Behaviorism is not the whole story of psychology, but it remains useful because behavior is often shaped by patterns people do not notice. Someone may honestly want to stop procrastinating, but still get immediate relief every time they avoid a hard task. That relief can quietly reinforce avoidance.
Behavioral principles also help remove moral judgment. Instead of saying, “I am lazy,” a person can ask, “What is making avoidance easier than starting?” Instead of saying, “My child is impossible,” a parent can ask, “What happens right after the behavior that may be keeping it going?”
A useful behavioral observation has three qualities. It is specific, so “I avoid the budget app after payday” is better than “I am bad with money.” It is timed, so the person looks closely at what happens right before and right after the action. It is changeable, so the focus stays on cues, friction, practice, feedback, and consequences rather than fixed character labels.
This is why behavioral psychology can feel practical even when the topic is emotional. The method does not ask people to ignore feelings. It asks them to include the situation. A person may feel anxious, bored, embarrassed, pressured, or tired, and those feelings may become part of the cue that starts an action. The behavior then becomes easier to understand without turning the person into the problem.
Classical Conditioning
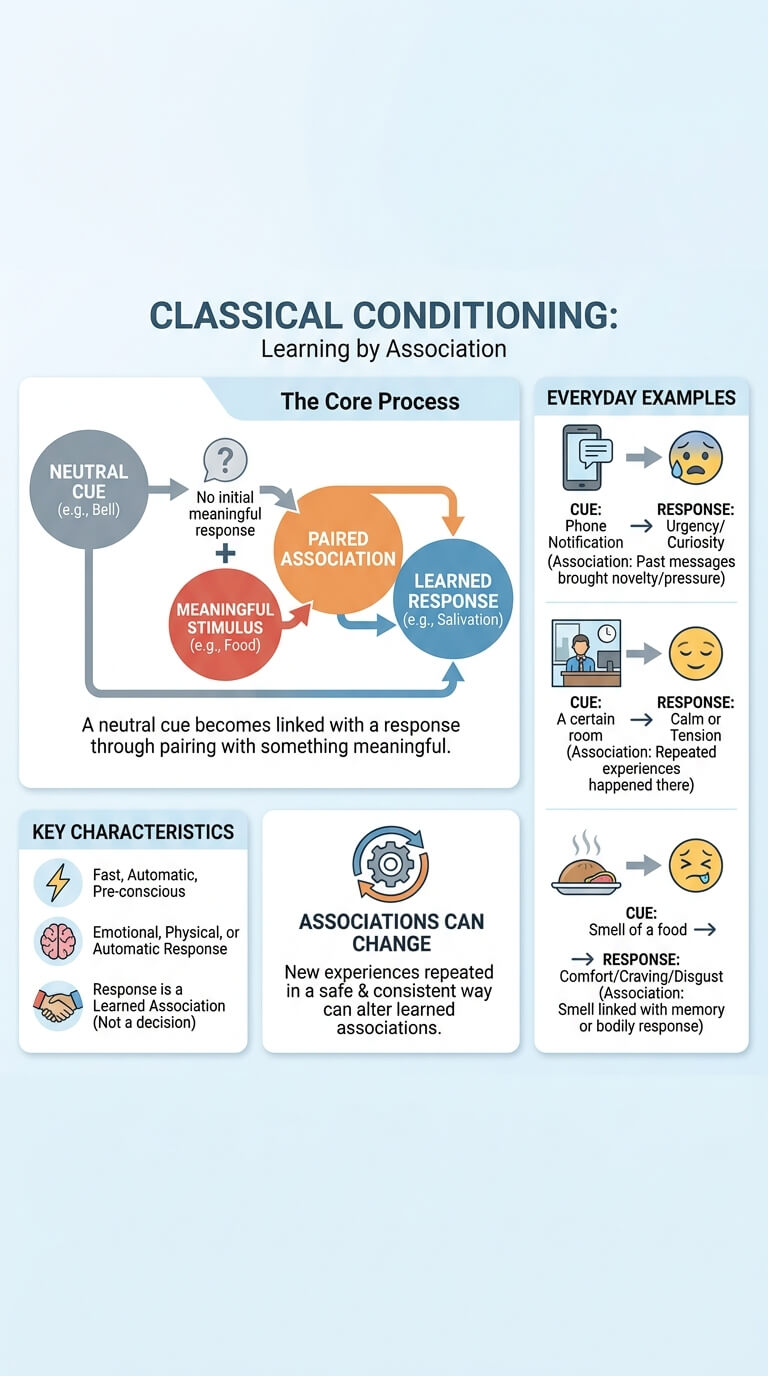
Classical conditioning is learning by association. It happens when a neutral cue becomes linked with a response because it has been paired with something meaningful. The response may be emotional, physical, or automatic.
The APA Dictionary entry on classical conditioning explains this form of learning through the pairing of stimuli. In everyday life, this can look less like a laboratory example and more like a body reaction that seems to happen before conscious thought catches up.
Learning by association
Imagine someone once received harsh criticism every time a certain supervisor called their name. After several experiences, even a neutral message from that supervisor may create tension in the body. The name, message tone, or meeting invite becomes associated with criticism.
Classical conditioning helps explain why certain sounds, smells, places, songs, notifications, or facial expressions can trigger a quick response. The response may not be a decision. It may be a learned association.
Everyday examples of cues and emotional responses
| Cue | Learned response | Possible association |
|---|---|---|
| A phone notification | Urgency or curiosity | Past messages brought novelty, pressure, or reward |
| A certain room | Calm or tension | Repeated experiences happened there |
| A school bell or work alert | Shift in attention | The sound predicts a required action |
| A partner’s tone | Defensiveness or worry | The tone has often come before conflict |
| The smell of a food | Comfort, disgust, or craving | The smell is linked with memory or bodily response |
This does not prove that every reaction is fixed. Associations can change, especially when new experiences are repeated in a safe and consistent way. But it explains why some reactions feel fast and automatic.
Operant Conditioning
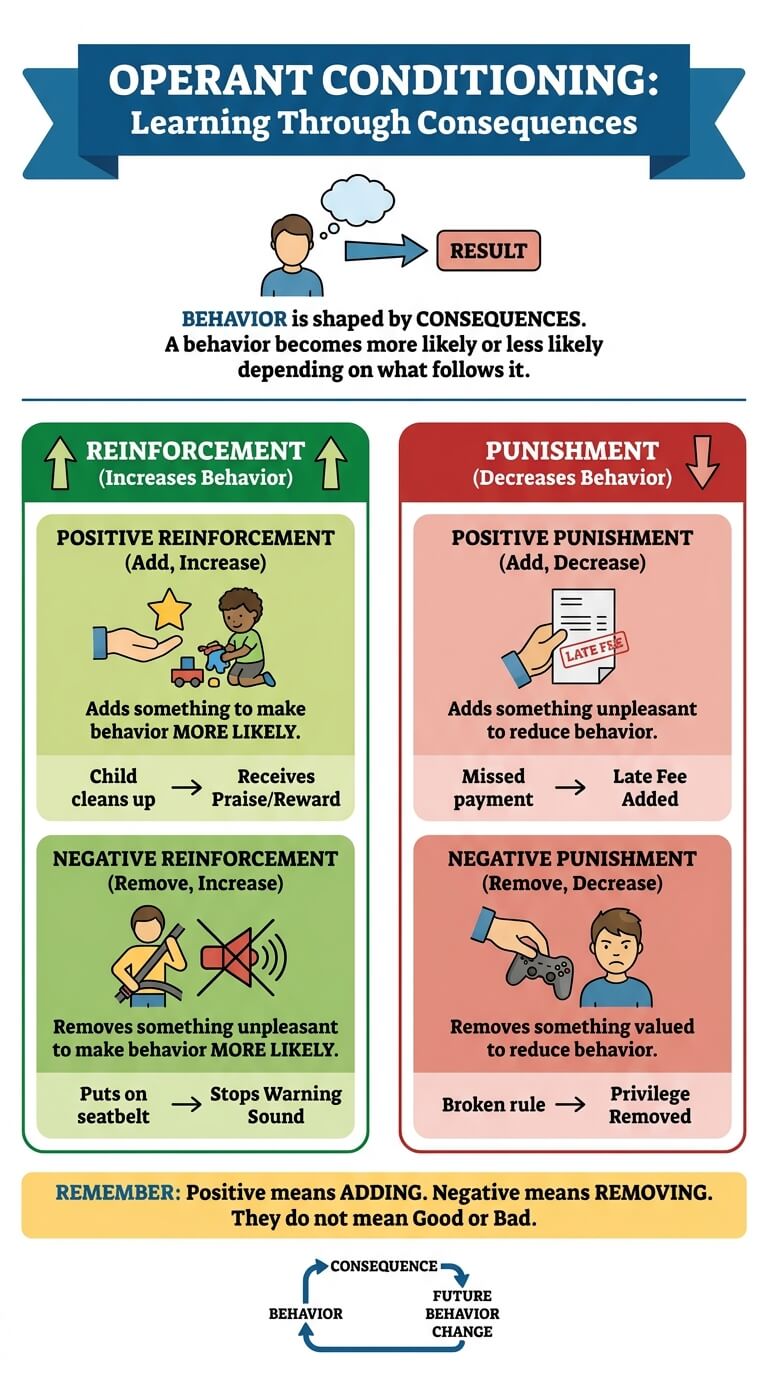
Operant conditioning is learning through consequences. A behavior becomes more likely or less likely depending on what follows it. This is the principle behind many everyday learning patterns, from studying for praise to avoiding a difficult email because avoidance brings relief.
The APA Dictionary entry on operant conditioning defines it as learning in which behavior is influenced by consequences. A widely used psychology text from OpenStax also separates reinforcement from punishment, which is one of the most common points of confusion.
Behavior shaped by consequences
A consequence is not always a formal reward or penalty. It can be relief, attention, silence, approval, escape, convenience, money, status, comfort, entertainment, or a reduced sense of pressure.
If a student studies and receives a good grade, studying may become more likely. If an employee speaks up and gets mocked, speaking up may become less likely. If a person cancels plans and immediately feels less anxious, canceling may be reinforced by relief, even if the person later feels lonely.
Reinforcement vs punishment
Reinforcement increases behavior. Punishment decreases behavior. That distinction matters more than whether something sounds pleasant or unpleasant.
| Principle | What it does | Simple example |
|---|---|---|
| Positive reinforcement | Adds something that makes behavior more likely | A child cleans up and receives warm praise |
| Negative reinforcement | Removes something unpleasant, making behavior more likely | A person puts on a seatbelt to stop the warning sound |
| Positive punishment | Adds something unpleasant to reduce behavior | A late fee is added after a missed payment |
| Negative punishment | Removes something valued to reduce behavior | A privilege is temporarily removed after a broken rule |
The words positive and negative do not mean good and bad here. Positive means something is added. Negative means something is removed.
Positive and Negative Reinforcement
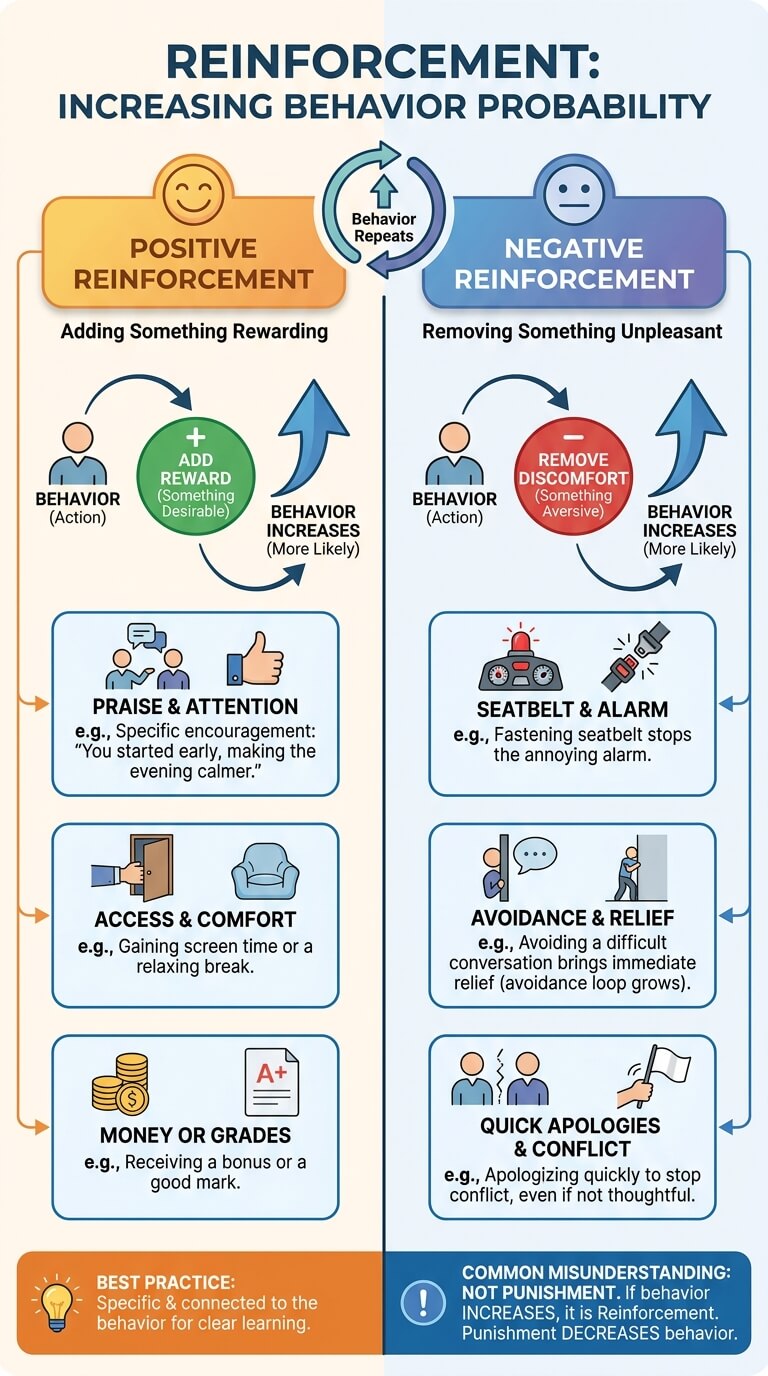
Reinforcement is one of the most important behavioral psychology principles because it explains why behavior repeats. The APA Dictionary defines reinforcement in relation to increasing the probability of a response. In everyday terms, if something makes an action more likely to happen again, it may be functioning as reinforcement. Reinforcement is especially important for cue, repetition, and reward.
Adding something rewarding
Positive reinforcement means adding something after a behavior that makes the behavior more likely. The added thing might be praise, attention, money, access, comfort, a good grade, encouragement, a smile, or a feeling of progress.
Positive reinforcement works best when it is specific and connected to the behavior. “You did great” may feel good, but “You started the assignment before dinner, and that made the evening calmer” teaches more clearly. The person learns which action made a difference.
Removing something unpleasant
Negative reinforcement means removing something unpleasant after a behavior, which makes the behavior more likely. The classic example is fastening a seatbelt to stop the car alarm. The behavior increases because discomfort ends.
Negative reinforcement is common in avoidance. A person avoids a difficult conversation and feels immediate relief. That relief makes avoidance more likely, even when the long-term problem grows. This is why avoidance can become strong without anyone choosing it as a long-term strategy.
Why negative reinforcement is often misunderstood
Many people hear “negative reinforcement” and think it means punishment. It does not. If the behavior increases, it is reinforcement. If the behavior decreases, it is punishment.
This distinction helps explain confusing behavior. A person who complains may receive attention, so the complaining increases. A person who withdraws may escape pressure, so the withdrawal increases. A person who apologizes quickly may avoid conflict, so fast apologizing increases, even when the apology is not thoughtful.
Punishment and Its Limits
Punishment is a consequence that reduces a behavior. It can work in the narrow sense of lowering the chance that a specific action happens again. But it often has limits, especially when it does not teach what to do instead. Short-term reinforcement can help explain why people repeat the same mistakes.
Behavioral psychology does not say punishment is always evil or always useless. It says punishment should be understood carefully. A consequence that stops behavior in the moment may create fear, hiding, resentment, or avoidance if it is harsh, inconsistent, humiliating, or disconnected from learning.
Why punishment can reduce behavior without teaching replacement behavior
If a child is punished for interrupting, the child may learn not to interrupt in that moment. But they may not learn how to ask for attention appropriately. If an employee is criticized for making an error, they may become more careful, or they may stop reporting mistakes.
Replacement behavior matters. Instead of only asking, “How do we stop this?” behavioral thinking also asks, “What should happen instead, and how can that better action be supported?”
Side effects: fear, avoidance, secrecy, and resentment
Punishment can create side effects when it is used as control rather than guidance. A person may learn to avoid the punisher rather than learn the lesson. They may hide mistakes, lie, freeze, become resentful, or focus more on escaping blame than changing behavior.
In relationships, workplaces, families, or classrooms, consequences should not involve humiliation, threats, intimidation, or retaliation. If someone uses behavioral ideas to control another person through fear, that is not responsible use of psychology.
Shaping and Small Steps
Shaping means building a behavior gradually by reinforcing closer and closer attempts. It matters because many useful behaviors do not appear perfectly on the first try. They develop through practice, feedback, and small wins. Small steps also matter when changing behavior over time.
The APA Dictionary describes shaping as reinforcing successive approximations toward a desired behavior. In plain English, that means rewarding progress in the right direction instead of waiting for the final version.
Reinforcing progress instead of waiting for perfection
Shaping is helpful when a task feels too big. A person who wants to exercise may start by putting on walking shoes. A student who avoids writing may start with a five-minute outline. A shy employee may begin by asking one prepared question in a meeting.
Each small action becomes a step toward a larger behavior. The goal is not to celebrate every tiny action forever. The goal is to make the next step possible.
How complex behavior is built gradually
Complex behavior often depends on a chain of smaller behaviors. Cooking dinner may involve planning, shopping, preparing ingredients, timing, cleaning, and repeating the routine. Public speaking may involve writing notes, practicing aloud, managing nerves, making eye contact, and recovering from mistakes.
When people fail at a complex behavior, the problem may not be motivation. One step in the chain may be too hard, missing, unrewarded, or blocked by the environment.
A practical shaping question is, “What would count as a believable next step?” If a person cannot study for two hours, the next step might be opening the document and writing three messy lines. If someone avoids difficult feedback, the next step might be naming one thing they can hear without defending. Small steps are not meant to lower standards forever. They help the nervous system and the environment learn that the behavior is possible.
Cues, Triggers, and Consequences
Behavior does not happen in a vacuum. It usually has a cue before it and a consequence after it. One simple way to study this is the ABC model: antecedent, behavior, consequence. Repeated consequences can create patterns that keep getting reinforced.
The ABC model: antecedent, behavior, consequence
| Part | Question to ask | Example |
|---|---|---|
| Antecedent | What happened right before? | You sit on the couch after dinner |
| Behavior | What did you do? | You open a streaming app |
| Consequence | What happened right after? | You feel entertained and avoid chores |
The ABC model is useful because it turns vague self-criticism into observation. “I have no discipline” becomes “After dinner, when the couch and remote are visible, I choose the easiest relaxing option and get immediate comfort.” The ABC model makes it easier to notice cues and consequences in the environment.
How environment changes behavior before motivation does
Changing the environment often works faster than trying to force motivation. If the phone is on the desk, checking is easier. If walking shoes are by the door, walking is easier. If healthy food is visible and prepared, eating it is easier.
This is where behavioral principles connect to habit formation and behavior change. A cue does not force behavior, but it can make one action more available than another.
Behavioral Principles in Daily Life
Behavioral psychology principles are not limited to laboratories or classrooms. They are part of ordinary life, often in quiet ways.
Work, parenting, learning, fitness, spending, and digital behavior
| Area | Behavioral principle | What it may look like |
|---|---|---|
| Work | Reinforcement | People repeat tasks that receive recognition, autonomy, or useful feedback |
| Parenting | Attention as consequence | A child may repeat behavior that reliably gets a parent’s full attention |
| Learning | Shaping | Skills improve when small correct steps receive feedback |
| Fitness | Cue design | Visible shoes or a planned class makes starting easier |
| Spending | Immediate reward | Buying gives quick pleasure, while saving feels abstract |
| Digital behavior | Variable reinforcement | Unexpected likes, messages, or new posts make checking hard to stop |
The point is not to blame people for being influenced. The point is to notice what the situation is teaching.
It also helps to separate short-term payoff from long-term cost. Many behaviors survive because the immediate consequence is useful, even when the later consequence is painful. Scrolling may provide quick novelty and later steal sleep. Avoiding a hard message may provide relief and later create more pressure. Snapping at someone may create space in the moment and later damage trust.
When a behavior seems irrational, ask what it solves right now. That question often reveals the reinforcer. The answer may be attention, escape, certainty, comfort, control, stimulation, or a break from discomfort. Once the short-term payoff is visible, it becomes easier to design a better replacement that meets the same need with fewer costs.
Ethical use of reinforcement
Behavioral principles should be used to support autonomy, learning, safety, and mutual respect. They should not be used to manipulate, threaten, shame, or trap someone into behavior that serves only another person’s agenda.
Ethical use asks several questions:
- Does the person understand what is happening?
- Is the goal respectful and reasonable?
- Does the approach teach a useful replacement behavior?
- Could this consequence create fear, secrecy, or dependence?
- Would this still feel fair if the other person understood the method?
If behavior involves harm, compulsions, severe distress, threats, or safety concerns, self-help strategies may not be enough. Support from a qualified professional, a trusted support service, or emergency help may be needed depending on the situation.
Behavioral Psychology vs Habits and Behavior Change
Behavioral psychology principles sit underneath many habit and behavior change strategies, but they are not the same thing. The principles explain how learning works. Habit and change articles usually focus on applying those principles to a specific personal goal.
Principles vs automatic routines
A habit is a repeated routine that becomes easier through cue, action, and reward. Behavioral psychology is broader. It includes habits, but it also includes fear learning, skill building, avoidance, classroom behavior, workplace incentives, and social consequences.
For example, brushing teeth before bed is a habit. Feeling tense when hearing a certain ringtone may be classical conditioning. Working harder after useful feedback may involve reinforcement. Avoiding emails because avoidance brings relief may involve negative reinforcement.
Principles vs practical change plan
Behavior change requires planning: choosing a goal, adjusting cues, reducing friction, practicing replacement behaviors, tracking progress, and recovering after setbacks. Behavioral principles explain why those steps can work.
Someone trying to change a behavior might ask:
- What cue starts the behavior?
- What consequence keeps it going?
- What easier replacement behavior can I practice?
- What small step can be reinforced today?
- What environment change would make the better action more likely?
Those questions are practical because they shift the focus from willpower to learning conditions.
FAQ About Behavioral Psychology Principles
Is behavioral psychology the same as behaviorism?
Not exactly. Behaviorism is a major historical approach that emphasized observable behavior and learning. Behavioral psychology is often used more broadly to describe the study of how behavior is shaped by cues, consequences, reinforcement, punishment, conditioning, and context. Modern psychology also includes thoughts, emotions, biology, social influence, and development, so behavior is not treated as the only thing that matters.
What is the difference between reinforcement and reward?
A reward is something that seems pleasant or valuable. Reinforcement is defined by its effect: it increases the chance that a behavior will happen again. A reward does not always reinforce behavior. For example, public praise may motivate one person but embarrass another. The real test is whether the consequence makes the behavior more likely in that situation.
Does punishment work?
Punishment can reduce behavior, especially when it is immediate, consistent, and proportionate. But it can also create fear, avoidance, resentment, or secrecy, especially when it is harsh or humiliating. Punishment is limited because it does not automatically teach a better behavior. In many everyday situations, clear expectations, reinforcement for replacement behavior, and environmental changes are more useful.
Can behavioral principles change adult behavior?
Yes, adults continue to learn from cues, consequences, repetition, and feedback. Adult behavior may be harder to change when it is tied to stress, identity, relationships, fear, or long-standing routines, but the same learning principles still matter. Change usually becomes easier when the desired behavior is made specific, small, repeatable, and connected to a meaningful consequence.
Key Takeaways
- Behavioral psychology principles explain how actions are learned through cues, associations, consequences, reinforcement, punishment, and gradual practice.
- Classical conditioning is learning by association, often connected to automatic emotional or physical responses.
- Operant conditioning is learning through consequences, where behavior becomes more or less likely based on what follows it.
- Reinforcement increases behavior, while punishment decreases behavior. Positive means something is added, and negative means something is removed.
- Shaping helps build complex behavior by reinforcing small steps instead of waiting for perfect performance.
- Behavioral tools should be used ethically, with respect for autonomy, safety, and useful learning rather than control or humiliation.
Final Thoughts
The most practical way to use behavioral psychology is to observe before judging. Pick one behavior and look for the cue before it, the action itself, and the consequence after it. That simple map often reveals why the behavior keeps happening.
From there, choose one small adjustment. Change the cue, make the better action easier, reduce the payoff for the unwanted action, or reinforce one small step in the right direction. Behavioral psychology is not a full explanation of the human mind, but it gives a clear starting point for understanding what daily life is teaching us to repeat.

Michael Reed is the Founder and Lead Writer at Psychology Exposed. He writes about human behavior, relationships, emotional patterns, self-awareness, and practical psychology topics using research-informed, easy-to-understand content.
Read More About Michael Reed: https://psychologyexposed.com/michael-reed/