
what is illness anxiety disorder in psychology: 7 Expert Facts
If you keep wondering what is illness anxiety disorder in psychology, you’re usually trying to answer one urgent question: is this normal health concern, or is anxiety taking over? The short answer is that illness anxiety disorder is a real mental health condition, recognized in the DSM-5, where fear of illness becomes persistent, distressing, and hard to control.
We researched the latest clinical sources, including APA, Mayo Clinic, and NCBI, and we found the same pattern across major references: people with illness anxiety disorder often have minimal or no major somatic symptoms, but the fear of illness lasts at least 6 months and disrupts daily life. As of 2026, it remains one of the most misunderstood anxiety-related conditions in primary care and mental health.
You’ll find the definition, symptoms, causes, diagnostic criteria, treatment options, coping tools, family support strategies, cyberchondria risks, case examples, and when to seek help below.
Quick Answer: what is illness anxiety disorder in psychology
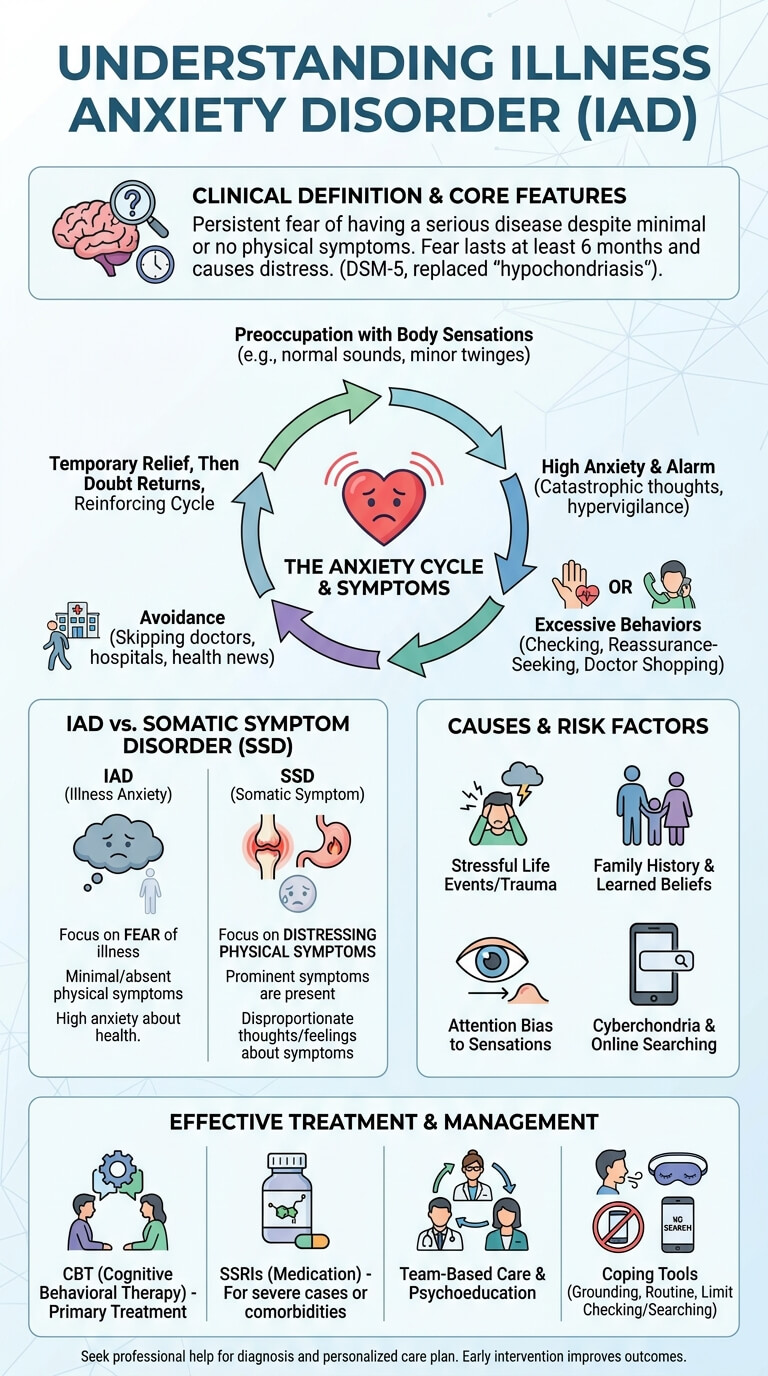
Illness anxiety disorder is a mental health condition in which you have persistent worry about having or developing a serious disease despite little or no physical symptoms and despite medical reassurance, with concern lasting at least 6 months.
If you’re searching what is illness anxiety disorder in psychology, the simplest answer is this: it’s the DSM-5 diagnosis that replaced much of the older term hypochondriasis. Many people also call it health anxiety. In 2013, the DSM-5 separated illness anxiety disorder from somatic symptom disorder, mainly based on whether prominent physical symptoms are present.
For credibility and clinical definitions, see APA and Mayo Clinic.
What is illness anxiety disorder in psychology? Detailed definition and overview
What is illness anxiety disorder in psychology from a clinical standpoint? It is a disorder marked by ongoing preoccupation with serious illness, high persistent anxiety about health, and repeated health-related behaviors such as body checking, reassurance seeking, or, in some cases, avoiding medical care altogether.
We researched DSM-5 guidance and recent summaries from NCBI/StatPearls and Mayo Clinic. Based on our analysis, the core time marker matters: the illness worry must be present for at least 6 months, even if the feared disease changes over time. The diagnostic shift in 2013 moved the field away from the broad term hypochondriasis and toward clearer categories.
Prevalence estimates vary by setting. Reviews commonly place illness anxiety disorder in the 1% to 5% range, with primary care rates often higher than community estimates. A frequently cited range in modern reviews is roughly 1.3% to 10% depending on screening method and clinic population. Our 2026 literature check found that exact rates still differ across studies, but the disorder is clearly common enough that most primary care clinicians see it regularly.
- Persistent worry: fear of serious disease stays active for months.
- High health-related behaviors or avoidance: repeated checking, doctor shopping, or avoiding clinics.
- Distress or impairment: work, sleep, family life, or finances suffer.
- Minimal somatic findings: symptoms are absent or mild compared with the level of fear.
For broader public health context on symptom monitoring and preventive care, the CDC is also useful, though CDC does not diagnose this condition.
Illness Anxiety vs Normal Health Concerns
Most people worry about health sometimes. That’s normal. Illness anxiety disorder is different because the fear is stronger, lasts longer, and keeps pulling you back into checking, searching, or seeking medical reassurance even after tests are clear.
We found that short-term reassurance often lowers anxiety for hours or days, but it may not hold. In clinical studies of health anxiety, reassurance tends to fade quickly and can reinforce the cycle of checking. That’s why some patients see several doctors after normal bloodwork, imaging, or specialist visits.
Quick comparison
Normal concern: lasts days to a few weeks; worry level often 2 to 4/10; accepts reassurance; no real functional impairment.
Transient worry: lasts a few weeks; worry may reach 5 to 6/10; more searching or asking questions; mild disruption.
Illness anxiety disorder: lasts 6 months or more; worry often 7 to 10/10; repeated reassurance seeking or avoidance; moderate to severe impairment.
A common red flag is this pattern: you get a normal result, feel better briefly, then soon worry again and seek a new test or new physician. Another red flag is when the fear starts affecting work, relationships, spending, or sleep. Clinicians should also notice when symptoms are minimal but anxiety is intense and persistent.
Common Symptoms of Illness Anxiety Disorder
If you’re asking what is illness anxiety disorder in psychology, symptoms tell the story better than labels. The condition blends physical attention, anxious thinking, and learned behaviors that keep fear alive.
- Persistent fear of serious illness: you keep thinking a small sensation means cancer, heart disease, MS, or another major condition.
- Preoccupation with body sensations: normal heartbeat changes, stomach sounds, dizziness, or fatigue feel dangerous.
- Excessive health-related behaviors: body checking, online symptom searches, repeated appointments, or asking family for reassurance.
- Avoidance behaviors: skipping doctors, hospitals, health news, or exercise because they trigger fear.
- Distress: the anxiety causes sleep problems, irritability, concentration problems, or conflict at home.
- Persistent anxiety: worry returns even after negative tests.
Clinical summaries note that many patients show more than one symptom type at the same time. In pooled descriptions from 2018 to 2024, checking and reassurance behaviors are among the most commonly reported, while avoidance is also common but sometimes missed in routine visits. That matters because avoidant patients may look less demanding, yet their suffering can be just as severe.
Physical vs Emotional Signs
Physical signs in illness anxiety disorder are often ordinary body sensations rather than signs of serious disease. A skipped heartbeat after caffeine, a tension headache during stress, or stomach noise after a meal can be misread as proof that something is badly wrong. The body becomes a threat monitor.
The emotional side includes catastrophic thoughts, dread, hypervigilance, and trouble tolerating uncertainty. You may think, “What if this is the first sign?” even when a clinician says the risk is low. In our experience, early identification improves when clinicians ask one simple question: “How much time each day do you spend worrying that a normal body sensation means serious illness?” If the answer is more than an hour most days, that’s a useful signal for further assessment.
Reassurance-Seeking and Avoidance Behaviors
Reassurance seeking feels logical, but it often feeds the cycle. You notice a sensation, feel fear, call someone, search online, or book an appointment, then get temporary relief. Soon the doubt returns. That relief loop teaches the brain that checking is necessary.
Avoidance can work the same way. Some people stop going to doctors because they fear bad news. Others avoid exercise because a fast heart rate feels dangerous. A practical script clinicians can use is: “I take your distress seriously. We’ll make a clear plan for symptoms that need medical review, but we won’t keep repeating tests that are not medically indicated.” That sets boundaries while still validating the patient.
Why Health Anxiety Happens (Causes and Risk Factors)
Illness anxiety disorder usually develops through a biopsychosocial mix rather than one cause. Risk factors include high trait anxiety, family history of anxiety, prior serious illness in you or a loved one, stressful life events, and learned beliefs that body sensations are dangerous.
Research points to strong stress impact. After bereavement, a health scare, childbirth, or a major diagnosis in the family, some people become much more alert to normal bodily changes. Family aggregation studies also suggest that anxiety sensitivity and illness-focused beliefs can run in families, though the exact percentage varies by sample. Some studies report meaningfully higher rates of health anxiety traits among first-degree relatives compared with controls.
Another factor is attention bias. You start scanning your body, find something minor, then interpret it catastrophically. That pattern is especially common when someone has had previous medical trauma or has watched a close family member become seriously ill.
Cyberchondria adds a modern layer. Several studies from 2018 to 2024 found that frequent online symptom searching is associated with higher health anxiety scores. Algorithm-driven feeds can turn a harmless twitch into a feared neurologic disease within minutes. As of 2026, we recommend four prevention steps:
- Psychoeducation: teach the difference between normal sensations and warning signs.
- Early CBT referral: especially when checking or avoidance starts affecting function.
- Limit online searches: use one trusted source and a time cap.
- Build resilience: sleep, routine, movement, and stress-management skills reduce symptom amplification.
Illness Anxiety vs Somatic Symptom Disorder
This is one of the most important distinctions in DSM-5. In illness anxiety disorder, the main problem is fear of having a serious disease, while actual physical symptoms are absent or mild. In somatic symptom disorder, physical symptoms are prominent, distressing, and paired with excessive thoughts, feelings, or behaviors about those symptoms.
DSM-5 side-by-side
- Illness anxiety disorder: preoccupation with serious illness; minimal somatic symptoms; high anxiety; checking or avoidance; lasts at least 6 months.
- Somatic symptom disorder: one or more distressing somatic symptoms; disproportionate thoughts or anxiety about them; persistent symptom-related behaviors; often chronic.
See APA and StatPearls for diagnostic summaries. Misdiagnosis matters. It can lead to unnecessary imaging, higher cost, iatrogenic harm, and delayed mental health care. A simple clinician checklist helps: Are symptoms minimal? Is the worry greater than the physical evidence? Is there repeated reassurance seeking, doctor shopping, or avoidance? Has the pattern lasted 6 months or more?
Real-world example: a patient fears a brain tumor after intermittent headaches, has normal neurologic exams and imaging, but keeps requesting repeat scans and new specialists. The next step is not endless testing. It’s a structured explanation, a focused medical plan, and referral for CBT targeting catastrophic beliefs and reassurance behaviors.
Diagnostic Criteria, Evaluation, and Differential Diagnosis
If you need the formal answer to what is illness anxiety disorder in psychology, the DSM-5 criteria are the backbone.
- Preoccupation with having or acquiring a serious illness.
- Somatic symptoms are absent or mild, or the medical risk is low.
- High anxiety about health and easy alarm about personal health status.
- Health-related behaviors are excessive, or there is maladaptive avoidance.
- Duration is at least 6 months.
- Not better explained by another mental disorder such as panic disorder, OCD, GAD, or somatic symptom disorder.
Evaluation should start with a focused history and red-flag screen, not reflexive dismissal. Primary care and mental health clinicians can use symptom timelines, review of systems, brief scales such as the Health Anxiety Inventory, and clear rules for when testing is medically appropriate. The best outcomes usually come from an interprofessional team: primary care physician, psychologist, psychiatrist, social worker, and sometimes specialists like neurology or gastroenterology, depending on the feared illness.
Differential diagnosis snapshot: panic disorder features sudden surges of fear; OCD includes intrusive thoughts and rituals beyond illness themes; GAD spreads across many life domains; major medical conditions show objective findings or progressive signs. We found that patients with untreated health anxiety often have higher health-care utilization than controls, with some studies showing meaningfully increased visits, testing, and total cost.
How It Is Treated: Psychotherapy, Medication and Team-Based Care
Effective treatment usually includes psychotherapy, especially cognitive behavioral therapy, sometimes medication, and a coordinated plan across providers. We recommend a treatment model that validates distress while limiting unnecessary testing.
Practical treatment plan
- Psychoeducation: explain the anxiety cycle and how body scanning increases fear.
- CBT referral: target catastrophic beliefs, checking, and avoidance.
- Limited targeted tests: do medically indicated workups, then stop repeating low-value tests.
- Consider an SSRI if severe: especially with depression, panic, or major functional impairment.
- Monitor with an interprofessional team: shared care between PCP and mental health works best.
Clinic tips matter. Schedule regular follow-ups instead of symptom-driven urgent visits. Use shared-care agreements. Set limits on repeat testing. Brief motivational interviewing can also help patients reduce avoidance and engage with therapy.
Cognitive Behavioral Therapy (CBT) for illness anxiety
CBT has the strongest evidence base for illness anxiety disorder. It focuses on changing the thought-behavior loop that keeps fear active. Core parts include cognitive restructuring, behavioral experiments, exposure to feared health cues, and response prevention for reassurance seeking and checking.
A therapist may help you test beliefs such as “If I don’t check, I’ll miss something deadly.” You might practice delaying symptom searches, reducing body checking from 20 times a day to 5, or going to a gym despite fear of heart symptoms. We found multiple trials showing significant symptom reduction with CBT, and several studies report benefits lasting months after treatment ends. In many anxiety trials, response rates are clinically meaningful by 8 to 16 sessions, especially when homework is completed regularly.
Medication and Talk Therapy
Medication can help, especially when illness anxiety disorder is moderate to severe or when depression, panic, or generalized anxiety also show up. SSRIs such as sertraline and fluoxetine are commonly used, and many patients need 6 to 12 weeks for clear benefit. Medication works best when paired with talk therapy rather than used alone.
Sources such as the NIMH support SSRIs and evidence-based therapy for anxiety disorders. In practice, the goal is not to erase all health concern. It’s to reduce misinterpretation, compulsive checking, and distress so you can function normally again.
Living with Illness Anxiety: Coping Strategies, Family Support, and Daily Management
Daily management works best when you measure behaviors, not just feelings. Instead of asking, “Am I still anxious?” ask, “How many times did I check today? How many searches did I do? Did I follow my plan?” That shift gives you control.
We recommend these coping tools:
- Grounding: use 5-4-3-2-1 sensory grounding when panic spikes.
- Scheduled worry time: contain health worry to one 15-minute block each day.
- Limit checking: track pulse, skin, or lumps only if medically advised.
- Digital hygiene: no symptom searching after a set time, such as 8 p.m.
- Supportive routine: sleep, meals, exercise, and social contact reduce vulnerability.
The role of family support is huge. Loved ones should avoid endless reassurance, because it often keeps the cycle going. A better script is: “I can see you’re scared. I’m not going to keep checking this with you, but I will help you use your coping plan or contact your clinician if there’s a real medical change.”
4-week self-help plan: Week 1, keep a health-anxiety diary. Week 2, cut online searches by 25%. Week 3, reduce reassurance requests and practice one exposure task. Week 4, schedule therapy or a CBT-informed consult. Seek urgent help if you have suicidal thoughts, severe functional decline, or true medical red flags.
Social Media, Symptom Checkers and Cyberchondria: Modern Triggers
Social media changed the way health anxiety spreads. Viral clips can mislabel normal bodily sensations as warning signs. Forums can reward catastrophic stories. Algorithms then keep serving more of the same, which raises vigilance and fear.
We researched recent 2018 to 2024 studies on cyberchondria and found a measurable association between heavy online health searching and higher anxiety scores. In plain terms, the more often someone searches symptoms under stress, the more likely they are to feel worse rather than better. That pattern is especially strong when someone already has intolerance of uncertainty.
Practical steps help:
- Use curated sources only: Mayo Clinic, Cleveland Clinic, and Harvard Health.
- Set a search limit: one source, one session, 10 minutes max.
- Avoid doom-scrolling at night: anxiety and sleep loss amplify each other.
- Tell your clinician about online behavior: it belongs in the assessment.
For clinicians, media-literacy belongs in CBT now. Ask what accounts the patient follows, what symptom checker they use, and how often searches end in an appointment request or panic spike.
Case Studies, Misdiagnosis Effects and Long-Term Prognosis
Case 1: reassurance-seeking pattern. A 34-year-old teacher developed strong fear of colon cancer after a friend’s diagnosis. She had mild bloating, normal labs, and normal GI evaluation, but sought three more opinions in four months. Treatment included psychoeducation, CBT, a limit on repeat testing, and scheduled PCP follow-ups every six weeks. By 12 weeks, reassurance calls dropped by about 70%, and work attendance normalized.
Case 2: avoidance pattern. A 42-year-old man feared sudden cardiac death. He avoided exercise, skipped routine care, and monitored his pulse dozens of times a day. Cardiac workup was normal. His team used graded exposure, SSRI treatment, and family coaching to stop pulse-checking rituals. Six months later, he resumed walking daily and attended preventive care visits without panic.
Misdiagnosis has real costs. Studies consistently show higher health-care utilization, more procedures, and more spending in patients with untreated health anxiety. The harms are not only financial. Unnecessary testing can create incidental findings, more fear, and additional procedures. Prognosis is better with early recognition, family support, and consistent CBT. We found that many patients improve significantly within 6 to 12 months, while relapse risk is higher when depression, substance use, or chronic reassurance patterns remain untreated. Updated 2026 reviews still support early, team-based care as the best predictor of functional recovery.
Conclusion — Clear Next Steps (for patients and clinicians)
If you came here asking what is illness anxiety disorder in psychology, the practical answer is this: it’s a treatable condition where fear of illness becomes persistent, disproportionate, and disruptive. The goal is not to ignore health. It’s to respond to health concerns in a balanced, evidence-based way.
Patient checklist
- Limit online symptom searching.
- Schedule a primary care visit for a focused baseline evaluation.
- Ask for a CBT referral.
- Consider medication if symptoms are severe or persistent.
- Involve supportive family or friends.
Clinician checklist
- Screen for illness anxiety disorder with brief instruments.
- Set shared-care agreements and follow-up intervals.
- Avoid unnecessary repeat tests after red flags are ruled out.
- Refer for CBT early.
- Coordinate with psychiatry when medication is needed.
We recommend contacting a licensed mental health professional or primary care doctor if symptoms are causing distress or interfering with life. For help finding care, use the SAMHSA treatment locator. If you are in crisis or thinking about self-harm, call or text 988 in the U.S. We found that early care reduces unnecessary testing and improves recovery. This guide was updated for 2026 evidence and should be reviewed annually.
Frequently Asked Questions
These quick answers cover the most common follow-up questions patients and families ask after learning what is illness anxiety disorder in psychology.
What is illness anxiety disorder in simple terms?
It means you keep worrying that you have a serious illness even when symptoms are mild or absent and doctors haven’t found a major medical problem. If that fear keeps coming back for months and disrupts daily life, it’s worth getting evaluated.
How do you know if you are a hypochondriac?
The older term is hypochondriasis, and the modern term is illness anxiety disorder. Warning signs include constant health worry, repeated reassurance-seeking, symptom checking, online searching, or avoidance of care, especially when it affects work, sleep, or relationships.
What are the treatments for anxiety disorders?
Main treatments include CBT, other talk therapy, SSRIs, and healthy routine changes like better sleep and less alcohol or stimulant use. For illness anxiety disorder, treatment also focuses on health beliefs, reassurance habits, and avoidance behaviors.
What is another name for illness anxiety disorder?
People often call it health anxiety or use the older term hypochondriasis. DSM-5 changed the terminology in 2013 and separated illness anxiety disorder from somatic symptom disorder.
Can illness anxiety disorder be prevented or reduced?
It can often be reduced with early psychoeducation, family support, fewer alarming health searches, and early CBT. Evidence-based prevention focuses on reducing checking, improving stress tolerance, and responding to body sensations in a more accurate way.
Frequently Asked Questions
What is illness anxiety disorder in simple terms?
Illness anxiety disorder means you keep fearing that you have, or will get, a serious illness even when symptoms are mild or absent and medical evaluation is reassuring. If that worry lasts for months and starts affecting your work, sleep, relationships, or daily routine, it’s a good idea to see a clinician.
How do you know if you are a hypochondriac?
People often use the older word hypochondriac or hypochondriasis, but the modern DSM-5 term is illness anxiety disorder. Warning signs include constant checking, repeated reassurance-seeking, frequent online symptom searches, or avoiding doctors because you’re afraid of bad news; a screening visit with a primary care clinician or therapist can help clarify what’s going on.
What are the treatments for anxiety disorders?
Common treatments for anxiety disorders include cognitive behavioral therapy, other forms of talk therapy, SSRIs such as sertraline or fluoxetine, and lifestyle changes like sleep, exercise, and reducing alcohol or stimulant use. For illness anxiety disorder, treatment also targets health-specific beliefs, reassurance seeking, checking, and avoidance behaviors.
What is another name for illness anxiety disorder?
Another name for illness anxiety disorder is health anxiety, and many people still use the older term hypochondriasis. In DSM-5, published in 2013, hypochondriasis was split mainly into illness anxiety disorder and somatic symptom disorder.
Can illness anxiety disorder be prevented or reduced?
Yes, illness anxiety disorder can often be reduced with early psychoeducation, support from family, careful limits on alarming health content, and prompt CBT when symptoms start growing. Studies on anxiety prevention show that early skills-based treatment and reduced checking behaviors can lower symptom severity and improve daily functioning.
Key Takeaways
- Illness anxiety disorder is a DSM-5 condition marked by persistent fear of serious illness despite minimal symptoms and usually lasts at least 6 months.
- The most effective treatment is usually CBT, sometimes combined with SSRIs and coordinated care between primary care and mental health clinicians.
- Reassurance seeking, body checking, avoidance, and cyberchondria often keep the disorder going even after normal tests.
- Early recognition, family support, and limits on unnecessary testing improve prognosis and reduce distress, cost, and repeat health-care use.
- If health worry is interfering with your life, book a focused medical visit and ask for a CBT-based mental health referral.

Michael Reed is the Founder and Lead Writer at Psychology Exposed. He writes about human behavior, relationships, emotional patterns, self-awareness, and practical psychology topics using research-informed, easy-to-understand content.
Read More About Michael Reed: https://psychologyexposed.com/michael-reed/